

QCA, IVUS and OCT in interventional cardiology in 2011
- PMID: 24282685
- PMCID: PMC3839131
- DOI: 10.3978/j.issn.2223-3652.2011.09.03
QCA, IVUS and OCT in interventional cardiology in 2011
Abstract
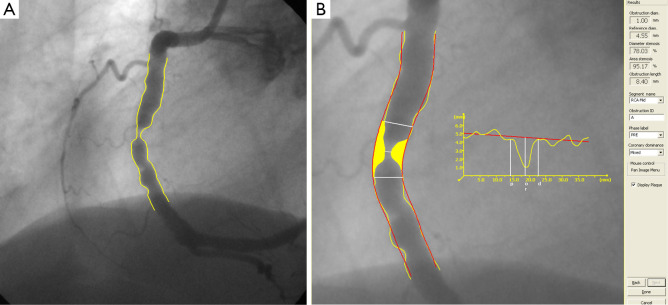
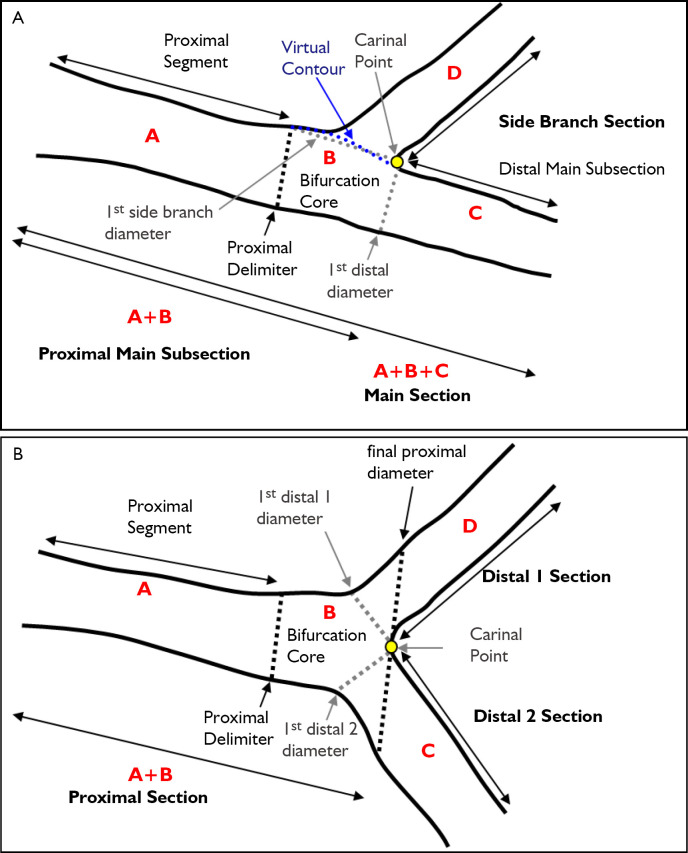
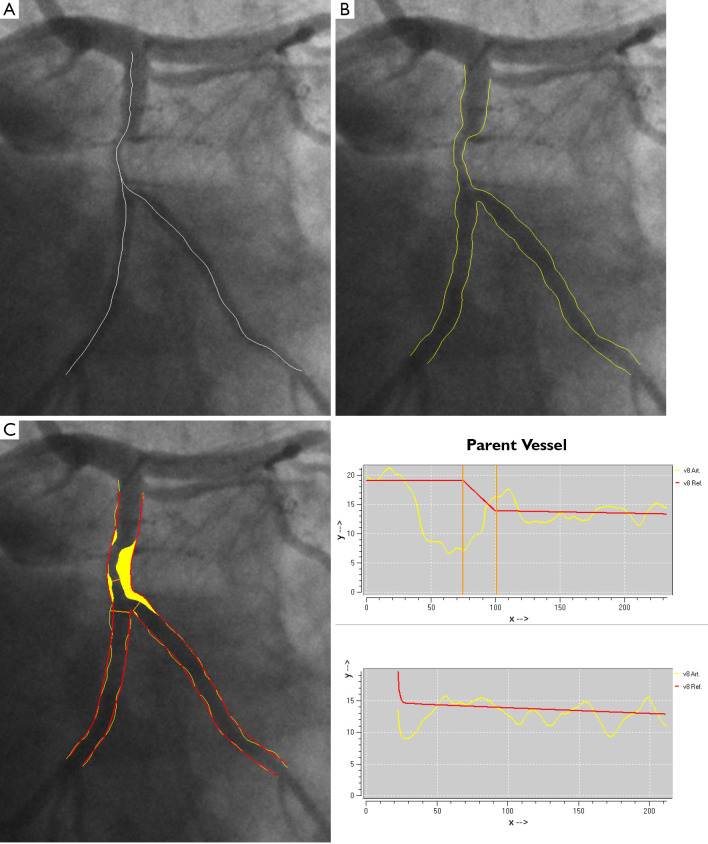
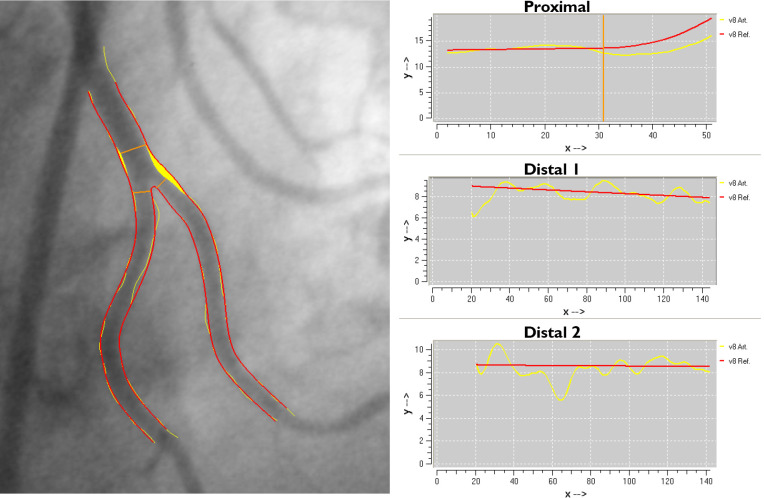
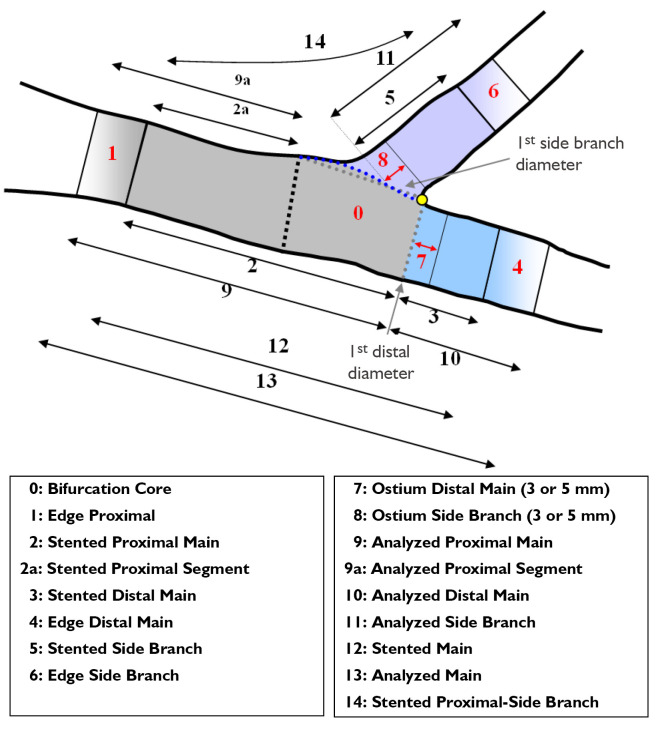
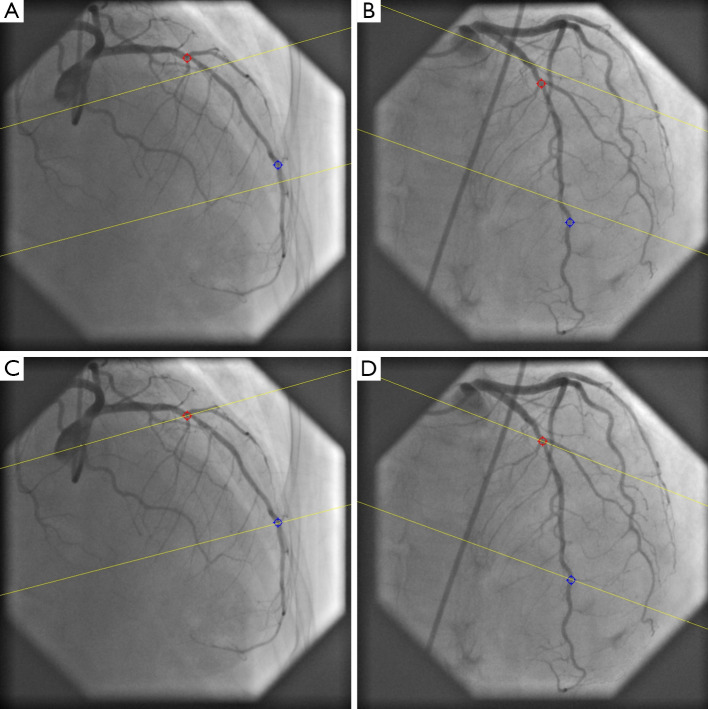
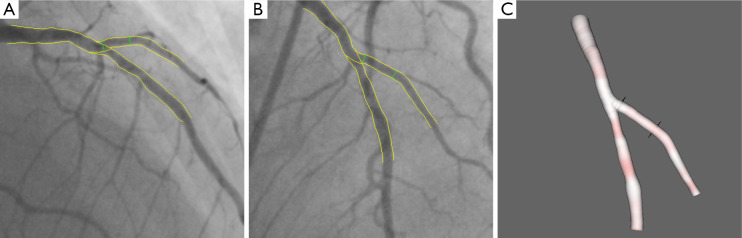
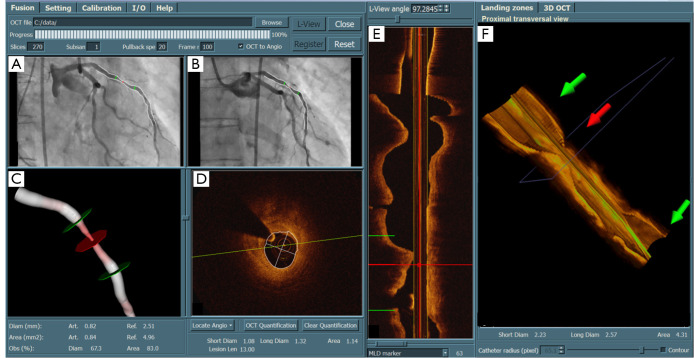
Over the past 30 years, quantitative coronary arteriography (QCA) has been used extensively as an objective and reproducible tool in clinical research to assess changes in vessel dimensions as a result of interventions, but also as a tool to provide evidence to the interventionalist prior to and after an intervention and at follow-up when necessary. With the increasing complexities of bifurcation stenting, corresponding analytical tools for bifurcation analysis have been developed with extensive reporting schemes. Although intravascular ultrasound (IVUS) has been around for a long time as well, more recent radiofrequency analysis provides additional information about the vessel wall composition; likewise optical coherence tomography (OCT) provides detailed information about the positions of the stent struts and the quality of the stent placement. Combining the information from the X-ray lumenogram and the intravascular imaging devices is mentally a challenging task for the interventionalist. To support the registration of these intravascular images with the X-ray images, 3D QCA has been developed and registered with the IVUS or OCT images, so that at every position along the vessel of interest the luminal data and the vessel wall data by IVUS or the stent strut data by OCT can be combined. From the 3D QCA the selection of the optimal angiographic views can also be facilitated. It is the intention of this overview paper to provide an extensive description of the techniques that we have developed and validated over the past 30 years.
Keywords: 3D reconstruction; Coronary artery disease; IVUS; OCT; QCA; registration.
Figures
References
-
- Reiber JH, Serruys PW, Kooijman CJ, et al. Assessment of short-, medium-, and long-term variations in arterial dimensions from computer-assisted quantitation of coronary cineangiograms. Circulation 1985;71:280-8. - PubMed
-
- Reiber JH, van der Zwet PM, Koning G, et al. Accuracy and precision of quantitative digital coronary arteriography: observer-, short-, and medium-term variabilities. Cathet Cardiovasc Diagn 1993;28:187-98. - PubMed
-
- Reiber JHC, Tuinenburg JC, Koning G, et al. Quantitative coronary arteriography. In: Coronary Radiology 2nd Revised Edition, Oudkerk M, Reiser MF (Eds.), Series: Medical Radiology, Sub series: Diagnostic Imaging, Baert AL, Knauth M, Sartor K (Eds.). Springer-Verlag, Berlin-Heidelberg 2009:41-65.
-
- Lansky A, Tuinenburg J, Costa M, et al. ; European Bifurcation Angiographic Sub-Committee. Quantitative angiographic methods for bifurcation lesions: a consensus statement from the European Bifurcation Group. Catheter Cardiovasc Interv 2009;73:258-66. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous