

Microbiota transplantation restores normal fecal bile acid composition in recurrent Clostridium difficile infection
- PMID: 24284963
- PMCID: PMC3920123
- DOI: 10.1152/ajpgi.00282.2013
Microbiota transplantation restores normal fecal bile acid composition in recurrent Clostridium difficile infection
Abstract
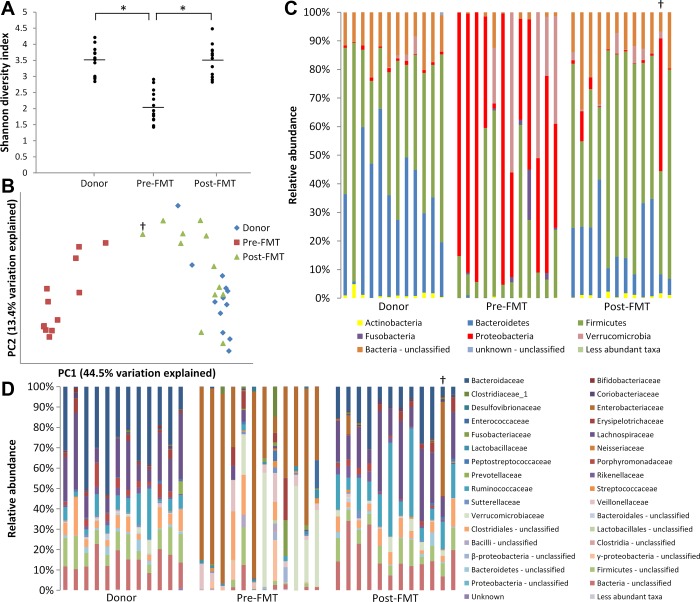
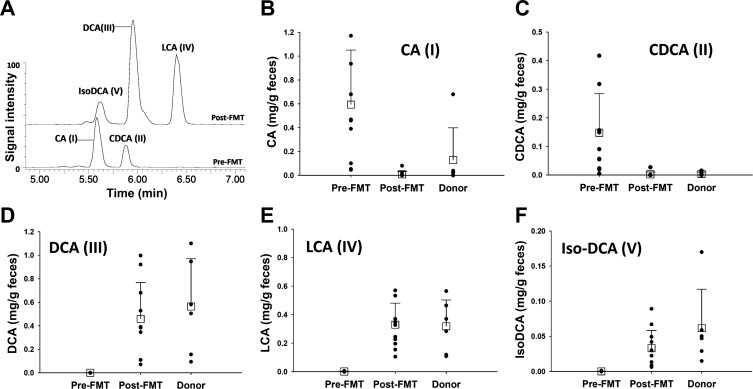
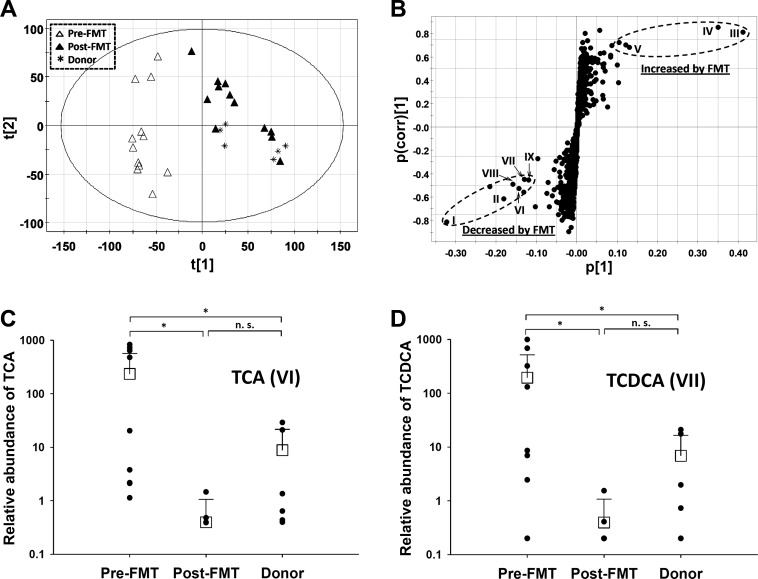
Fecal microbiota transplantation (FMT) has emerged as a highly effective therapy for refractory, recurrent Clostridium difficile infection (CDI), which develops following antibiotic treatments. Intestinal microbiota play a critical role in the metabolism of bile acids in the colon, which in turn have major effects on the lifecycle of C. difficile bacteria. We hypothesized that fecal bile acid composition is altered in patients with recurrent CDI and that FMT results in its normalization. General metabolomics and targeted bile acid analyses were performed on fecal extracts from patients with recurrent CDI treated with FMT and their donors. In addition, 16S rRNA gene sequencing was used to determine the bacterial composition of pre- and post-FMT fecal samples. Taxonomic bacterial composition of fecal samples from FMT recipients showed rapid change and became similar to the donor after the procedure. Pre-FMT fecal samples contained high concentrations of primary bile acids and bile salts, while secondary bile acids were nearly undetectable. In contrast, post-FMT fecal samples contained mostly secondary bile acids, as did non-CDI donor samples. Therefore, our analysis showed that FMT resulted in normalization of fecal bacterial community structure and metabolic composition. Importantly, metabolism of bile salts and primary bile acids to secondary bile acids is disrupted in patients with recurrent CDI, and FMT corrects this abnormality. Since individual bile salts and bile acids have pro-germinant and inhibitory activities, the changes suggest that correction of bile acid metabolism is likely a major mechanism by which FMT results in a cure and prevents recurrence of CDI.
Keywords: Clostridium difficile; bile acids; fecal microbiota transplantation.
Figures
References
-
- Ananthakrishnan AN. Clostridium difficile infection: epidemiology, risk factors and management. Nat Rev Gastroenterol Hepatol 8: 17–26, 2011 - PubMed
-
- Arumugam M, Raes J, Pelletier E, Le Paslier D, Yamada T, Mende DR, Fernandes GR, Tap J, Bruls T, Batto JM, Bertalan M, Borruel N, Casellas F, Fernandez L, Gautier L, Hansen T, Hattori M, Hayashi T, Kleerebezem M, Kurokawa K, Leclerc M, Levenez F, Manichanh C, Nielsen HB, Nielsen T, Pons N, Poulain J, Qin J, Sicheritz-Ponten T, Tims S, Torrents D, Ugarte E, Zoetendal EG, Wang J, Guarner F, Pedersen O, de Vos WM, Brunak S, Dore J, Antolin M, Artiguenave F, Blottiere HM, Almeida M, Brechot C, Cara C, Chervaux C, Cultrone A, Delorme C, Denariaz G, Dervyn R, Foerstner KU, Friss C, van de Guchte M, Guedon E, Haimet F, Huber W, van Hylckama-Vlieg J, Jamet A, Juste C, Kaci G, Knol J, Lakhdari O, Layec S, Le Roux K, Maguin E, Merieux A, Melo Minardi R, M'Rini C, Muller J, Oozeer R, Parkhill J, Renault P, Rescigno M, Sanchez N, Sunagawa S, Torrejon A, Turner K, Vandemeulebrouck G, Varela E, Winogradsky Y, Zeller G, Weissenbach J, Ehrlich SD, Bork P. Enterotypes of the human gut microbiome. Nature 473: 174–180, 2011 - PMC - PubMed
-
- Borody TJ, Khoruts A. Fecal microbiota transplantation and emerging applications. Nat Rev Gastroenterol Hepatol 9: 88–96, 2011 - PubMed
-
- Carman RJ, Simon MA, Petzold HE, 3rd, Wimmer RF, Batra MR, Fernandez AH, Miller MA, Bartholomew M. Antibiotics in the human food chain: establishing no effect levels of tetracycline, neomycin, and erythromycin using a chemostat model of the human colonic microflora. Regul Toxicol Pharmacol 43: 168–180, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical