

Prevalence of ataxia in children: a systematic review
- PMID: 24285620
- PMCID: PMC3873624
- DOI: 10.1212/01.wnl.0000438224.25600.6c
Prevalence of ataxia in children: a systematic review
Abstract
Objective: To estimate the prevalence of childhood ataxia resulting from both genetic and acquired causes.
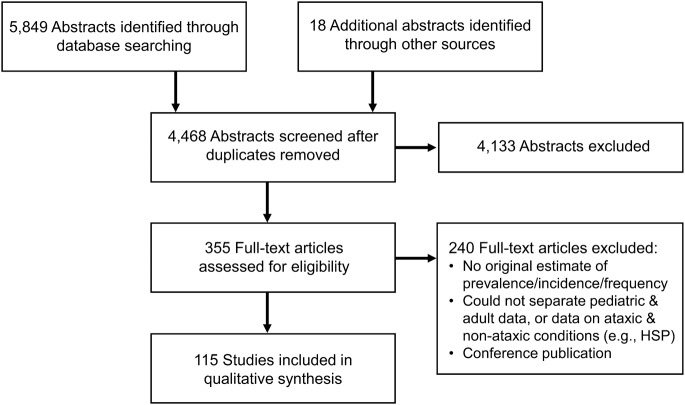
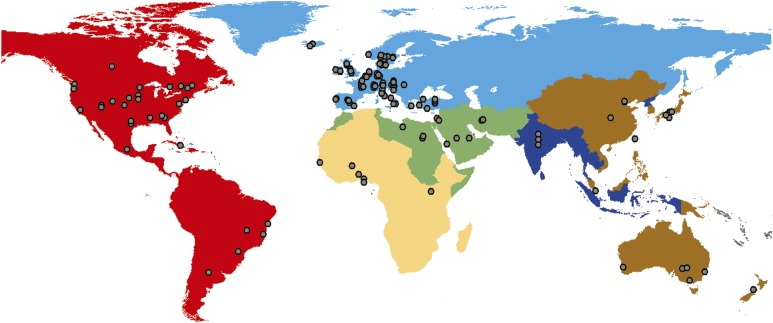
Methods: A systematic review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement. Five databases were searched for articles reporting a frequency measure (e.g., prevalence, incidence) of ataxia in children. Included articles were first grouped according to the World Health Organization (WHO) regions and subsequently classified according to etiology (genetic, acquired, or mixed). Each article was assessed for its risk of bias on the domains of sampling, measurement, and analysis. Incidence values were converted to prevalence estimates whenever possible. European prevalence estimates for different etiologies of ataxia were summed to gauge the overall prevalence of childhood ataxia.
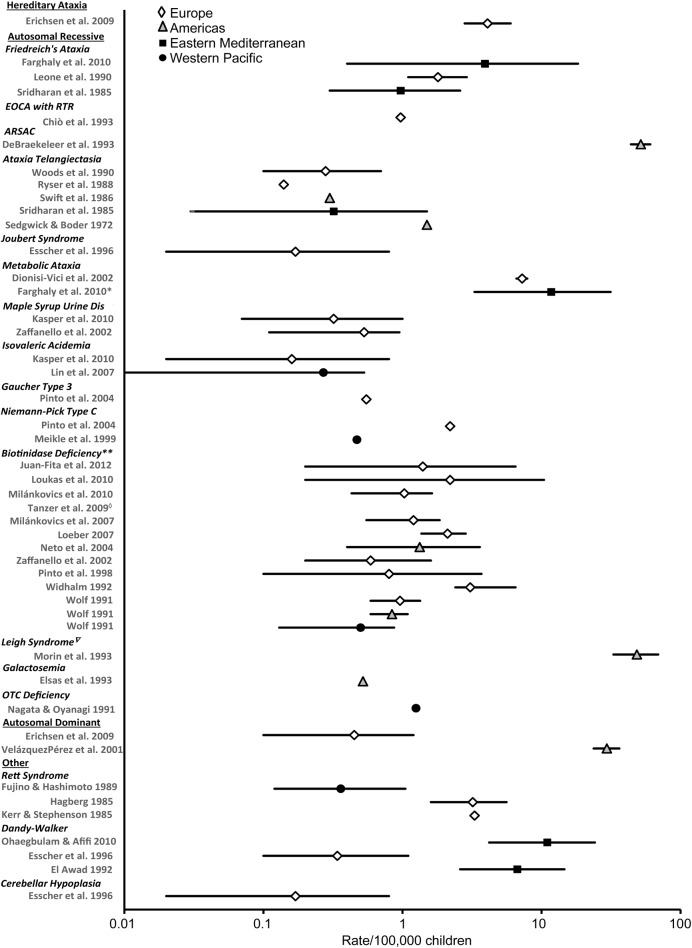
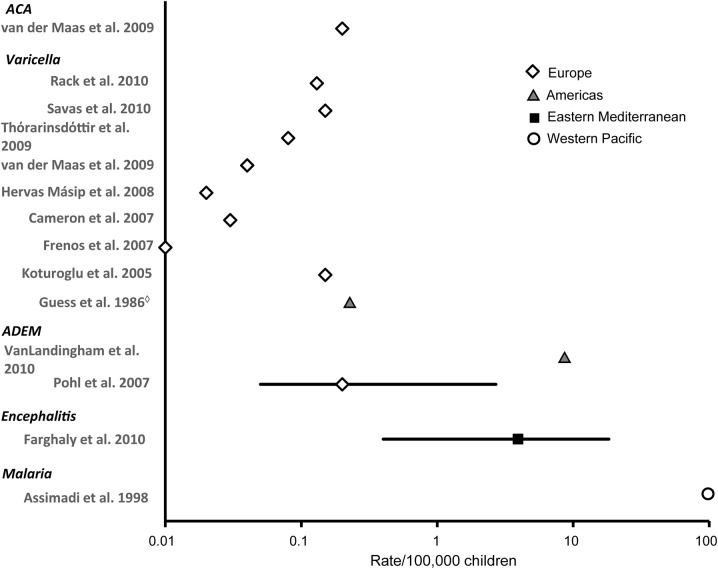
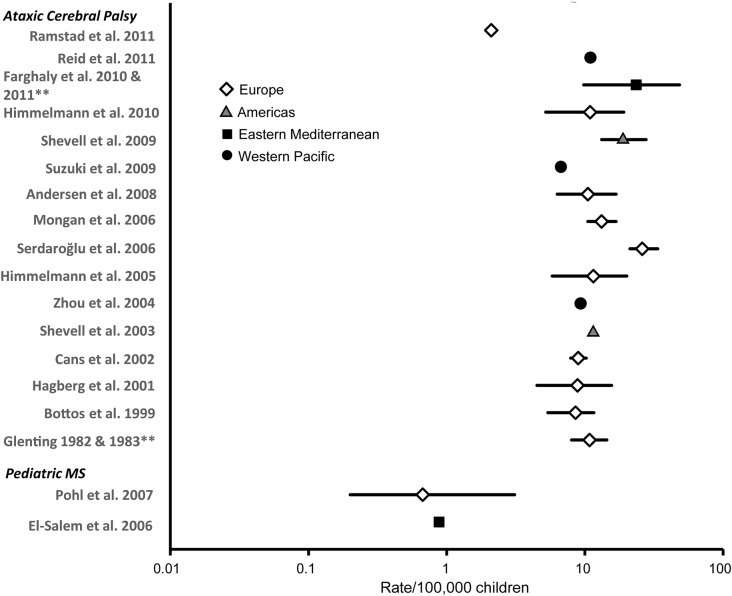
Results: One hundred fifteen articles were included in the review. More than 50% of the data originated from the Europe WHO region. Data from this region also showed the least susceptibility to bias. Little data were available for Africa and Southeast Asia. The prevalence of acquired ataxias was found to vary more greatly across regions than the genetic ataxias. Ataxic cerebral palsy was found to be a significant contributor to the overall prevalence of childhood ataxia across WHO regions. The prevalence of childhood ataxias in Europe was estimated to be ∼26/100,000 children and likely reflects a minimum prevalence worldwide.
Conclusions: The findings show that ataxia is a common childhood motor disorder with a higher prevalence than previously assumed. More research concerning the epidemiology, assessment, and treatment of childhood ataxia is warranted.
Figures
References
-
- Manto MU. Clinical signs of cerebellar disorders. In: Manto MU, Pandolfo M, editors. The Cerebellum and Its Disorders. Cambridge: Cambridge University Press; 2002:97–120
-
- Konczak J, Timmann D. The effect of damage to the cerebellum on sensorimotor and cognitive function in children and adolescents. Neurosci Biobehav Rev 2007;31:1101–1113 - PubMed
-
- Ryan MM, Engle EC. Acute ataxia in childhood. J Child Neurol 2003;18:309–316 - PubMed
-
- Leone M, Brignolio F, Rosso MG, et al. Friedreich's ataxia: a descriptive epidemiological study in an Italian population. Clin Genet 1990;38:161–169 - PubMed
-
- Werdelin L, Keiding N. Hereditary ataxias: epidemiological aspects. Neuroepidemiology 1990;9:321–331 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical