

Prevalence, risk factors, and uptake of interventions for sexually transmitted infections in Britain: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal)
- PMID: 24286785
- PMCID: PMC3899025
- DOI: 10.1016/S0140-6736(13)61947-9
Prevalence, risk factors, and uptake of interventions for sexually transmitted infections in Britain: findings from the National Surveys of Sexual Attitudes and Lifestyles (Natsal)
Abstract
Background: Population-based estimates of prevalence, risk distribution, and intervention uptake inform delivery of control programmes for sexually transmitted infections (STIs). We undertook the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3) after implementation of national sexual health strategies, and describe the epidemiology of four STIs in Britain (England, Scotland, and Wales) and the uptake of interventions.
Methods: Between Sept 6, 2010 and Aug 31, 2012, we did a probability sample survey of 15,162 women and men aged 16-74 years in Britain. Participants were interviewed with computer-assisted face-to-face and self-completion questionnaires. Urine from a sample of participants aged 16-44 years who reported at least one sexual partner over the lifetime was tested for the presence of Chlamydia trachomatis, type-specific human papillomavirus (HPV), Neisseria gonorrhoeae, and HIV antibody. We describe age-specific and sex-specific prevalences of infection and intervention uptake, in relation to demographic and behavioural factors, and explore changes since Natsal-1 (1990-91) and Natsal-2 (1999-2001).
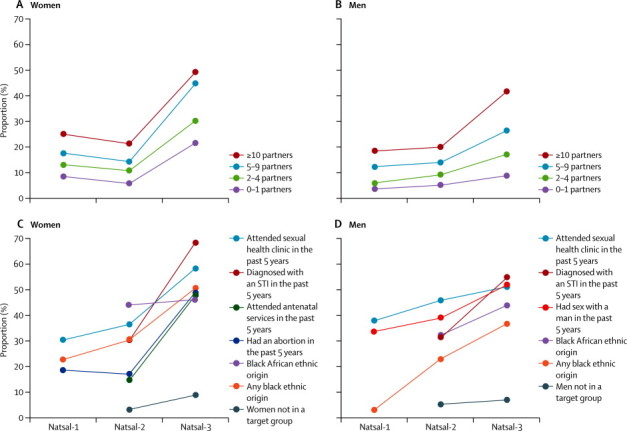
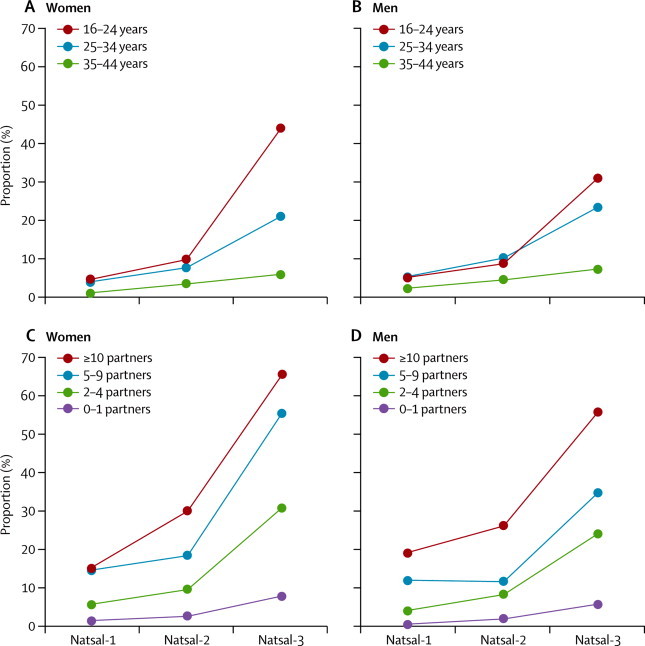
Findings: Of 8047 eligible participants invited to provide a urine sample, 4828 (60%) agreed. We excluded 278 samples, leaving 4550 (94%) participants with STI test results. Chlamydia prevalence was 1·5% (95% CI 1·1-2·0) in women and 1·1% (0·7-1·6) in men. Prevalences in individuals aged 16-24 years were 3·1% (2·2-4·3) in women and 2·3% (1·5-3·4) in men. Area-level deprivation and higher numbers of partners, especially without use of condoms, were risk factors. However, 60·4% (45·5-73·7) of chlamydia in women and 43·3% (25·9-62·5) in men was in individuals who had had one partner in the past year. Among sexually active 16-24-year-olds, 54·2% (51·4-56·9) of women and 34·6% (31·8-37·4) of men reported testing for chlamydia in the past year, with testing higher in those with more partners. High-risk HPV was detected in 15·9% (14·4-17·5) of women, similar to in Natsal-2. Coverage of HPV catch-up vaccination was 61·5% (58·2-64·7). Prevalence of HPV types 16 and 18 in women aged 18-20 years was lower in Natsal-3 than Natsal-2 (5·8% [3·9-8·6] vs 11·3% [6·8-18·2]; age-adjusted odds ratio 0·44 [0·21-0·94]). Gonorrhoea (<0·1% prevalence in women and men) and HIV (0·1% prevalence in women and 0·2% in men) were uncommon and restricted to participants with recognised high-risk factors. Since Natsal-2, substantial increases were noted in attendance at sexual health clinics (from 6·7% to 21·4% in women and from 7·7% to 19·6% in men) and HIV testing (from 8·7% to 27·6% in women and from 9·2% to 16·9% in men) in the past 5 years.
Interpretation: STIs were distributed heterogeneously, requiring general and infection-specific interventions. Increases in testing and attendance at sexual health clinics, especially in people at highest risk, are encouraging. However, STIs persist both in individuals accessing and those not accessing services. Our findings provide empirical evidence to inform future sexual health interventions and services.
Funding: Grants from the UK Medical Research Council and the Wellcome Trust, with support from the Economic and Social Research Council and the Department of Health.
Copyright © 2013 Sonnenberg et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Epidemiology: Largest national survey offers insight into sexual health in Britain.Nat Rev Urol. 2014 Jan;11(1):1. doi: 10.1038/nrurol.2013.304. Epub 2013 Dec 17. Nat Rev Urol. 2014. PMID: 24346011 No abstract available.
References
-
- Public Health England Health Protection Report. June 7, 2013. http://www.hpa.org.uk/hpr/archives/2013/hpr2313.pdf (accessed Nov 5, 2013).
-
- Johnson AM, Wadsworth J, Wellings K, Field J. The National Survey of Sexual Attitudes and Lifestyles. Blackwell Scientific Press; Oxford: 1994.
-
- Johnson AM, Mercer CH, Erens B. Sexual behaviour in Britain: partnerships, practices, and HIV risk behaviours. Lancet. 2001;358:1835–1842. - PubMed
-
- Fenton KA, Korovessis C, Johnson AM. Sexual behaviour in Britain: reported sexually transmitted infections and prevalent genital Chlamydia trachomatis infection. Lancet. 2001;358:1851–1854. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
