

Recompression in new levels after percutaneous vertebroplasty and kyphoplasty compared with conservative treatment
- PMID: 24287674
- PMCID: PMC3889698
- DOI: 10.1007/s00402-013-1886-3
Recompression in new levels after percutaneous vertebroplasty and kyphoplasty compared with conservative treatment
Abstract
Study design: A prospective clinical study assessing new vertebral compression fracture after previous treatment.
Objective: The purpose of this study was to investigate the incidence and associated risk factors of new symptomatic osteoporotic vertebral compression fractures (OVCFs) in patients treated by percutaneous vertebroplasty (PVP) and kyphoplasty (PKP) versus conservative treatment, and to elucidate our findings. There are a lot of reports concerning the feasibility and efficacy of this minimally invasive procedure compared with conservative treatment, especially in pain soothing. However, it is still unclear whether the risk of subsequent fracture has increased among operative treatment patients in the long term.
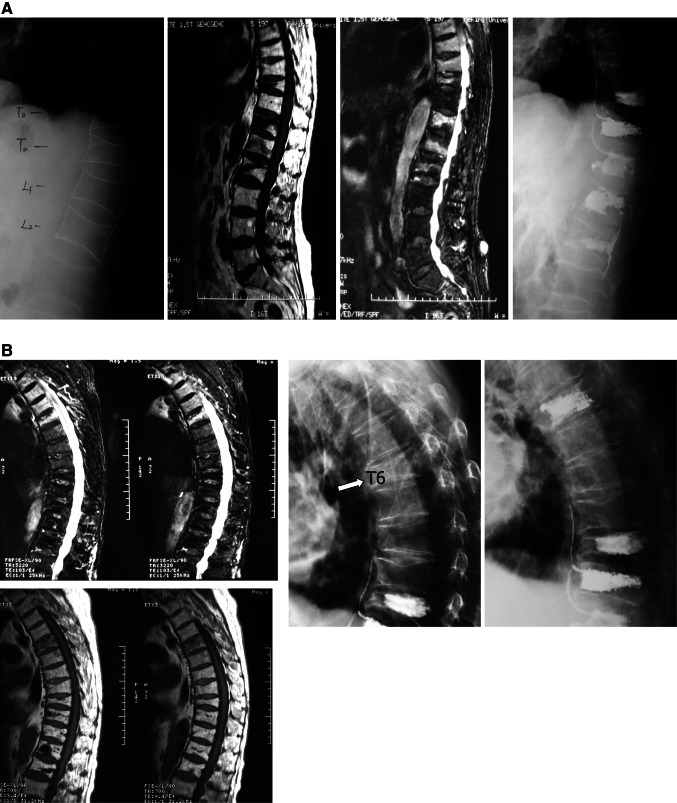
Methods: From November 2005 to July 2009, 290 consecutive patients with 363 OVCFs were randomly selected for PVP/PKP or conservative treatment and evaluated with a mean follow-up of 49.4 months (36-80 months). Some parameters were characterized and statistically compared in this study. Telephone questionnaires, clinical reexamine, and plain radiographs were performed in the follow-up.
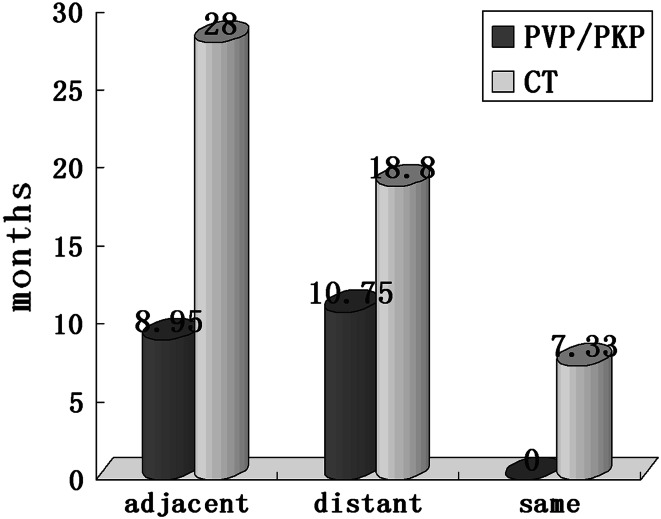
Results: Thirty-one of 290 (10.7%) patients had experienced 42 newly developed symptomatic secondary OVCFs. Among 169 operation (53.3% vertebroplasty, 46.7% kyphoplasty) and 121 comparison patients, there is no significant statistical difference of new OVCFs incidence between the two groups calculated by patient proportion. However, in separate, the rate of secondary adjacent fractures calculated by vertebral refracture number is significantly higher than non-adjacent levels in PVP/PKP group but no significant statistical difference was observed in conservative group. The time interval of recompression after operative procedure was much shorter than that for comparison group (9.7 ± 17.8 versus 22.4 ± 7.99 months, p = 0.017). In addition, older age, gender, fracture times, location of original fracture segment, the amount of cement, cement leakage, operation modality (PVP or PKP),and initial number of OVCFs were documented, but these were not the influencing factors in this study (p > 0.05).
Conclusions: Patients who had experienced PVP/PKP were not associated with an increased risk of recompression in new levels. However, recompression in new levels of PVP/PKP group occurred much sooner than that of conservative group in the follow-up period. The incidence of new vertebral fractures observed at adjacent levels was substantially higher but no sooner than at distant levels in PVP/PKP group. No major risk factors involving new OVCFs have been found in this study and augmentation for sandwich situation is not necessary.
Figures
References
-
- Galibert P, Deramond H, Rosat P, et al. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33:166–168. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
