

MRI in necrotizing fasciitis of the extremities
- PMID: 24288403
- PMCID: PMC3898976
- DOI: 10.1259/bjr.20130560
MRI in necrotizing fasciitis of the extremities
Abstract
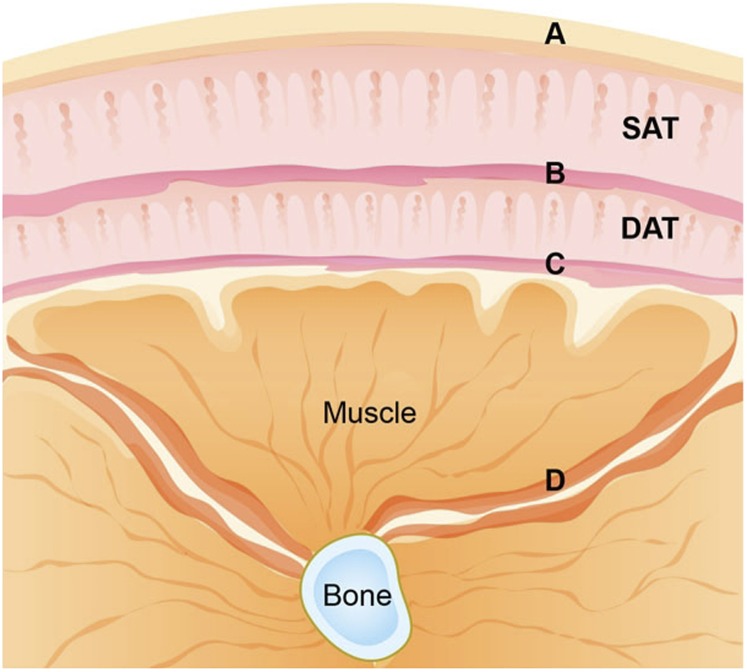
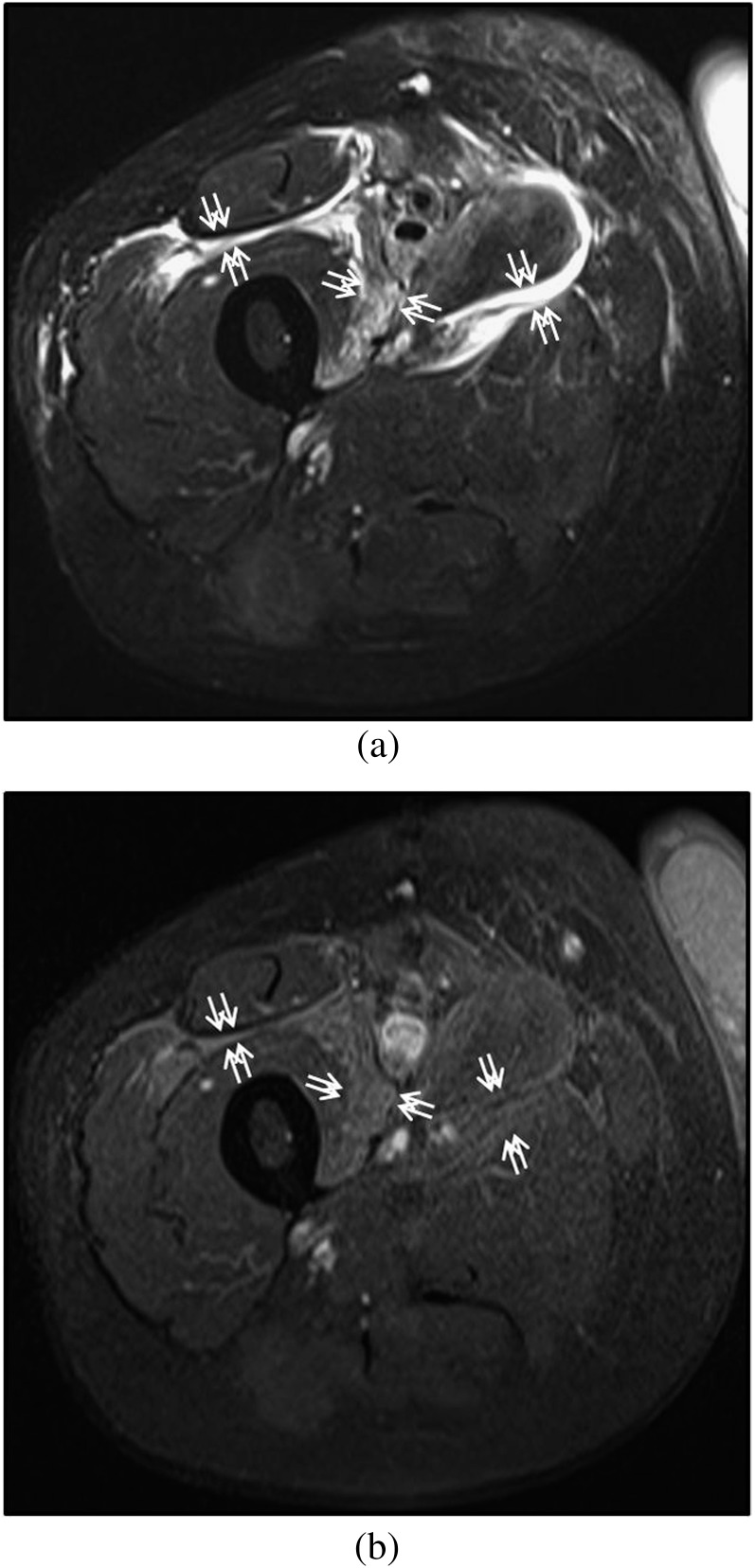
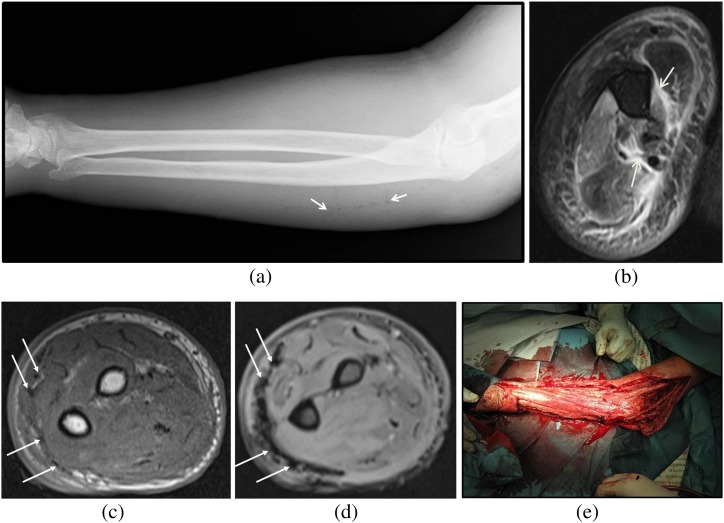
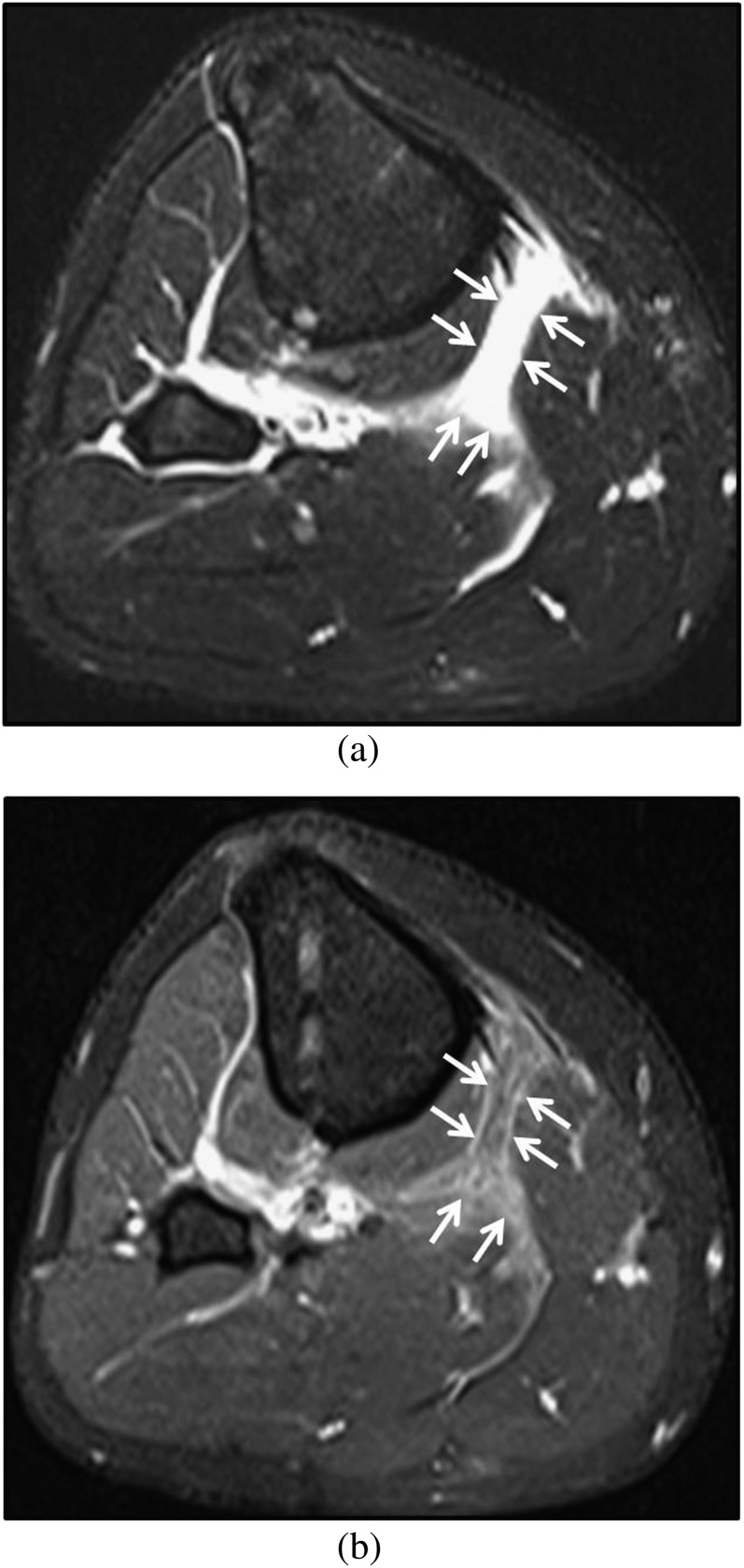
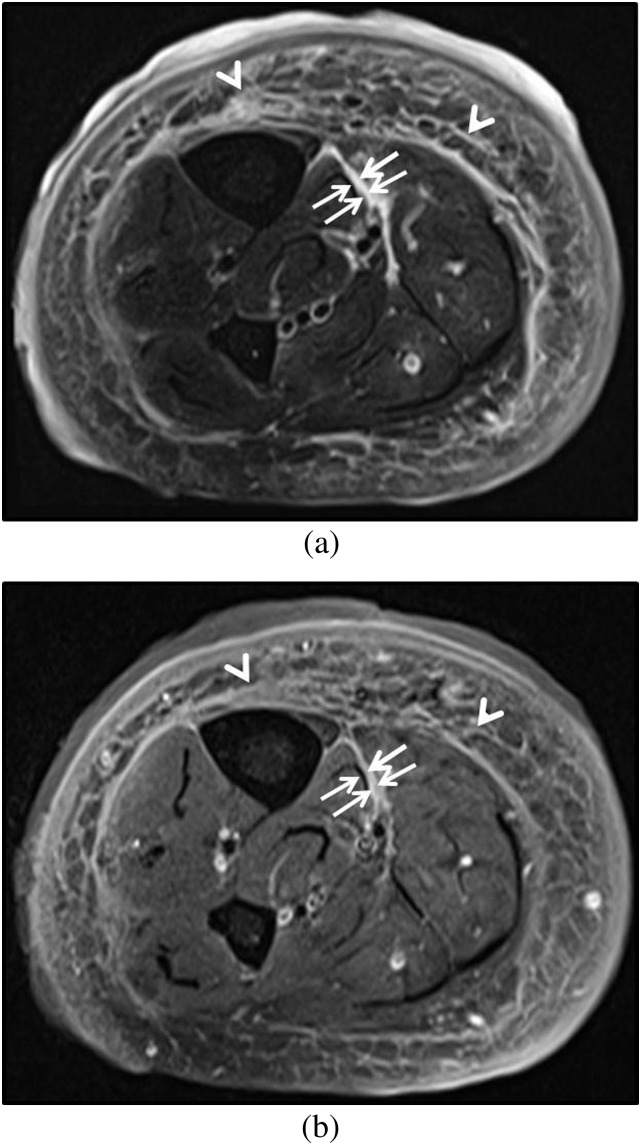
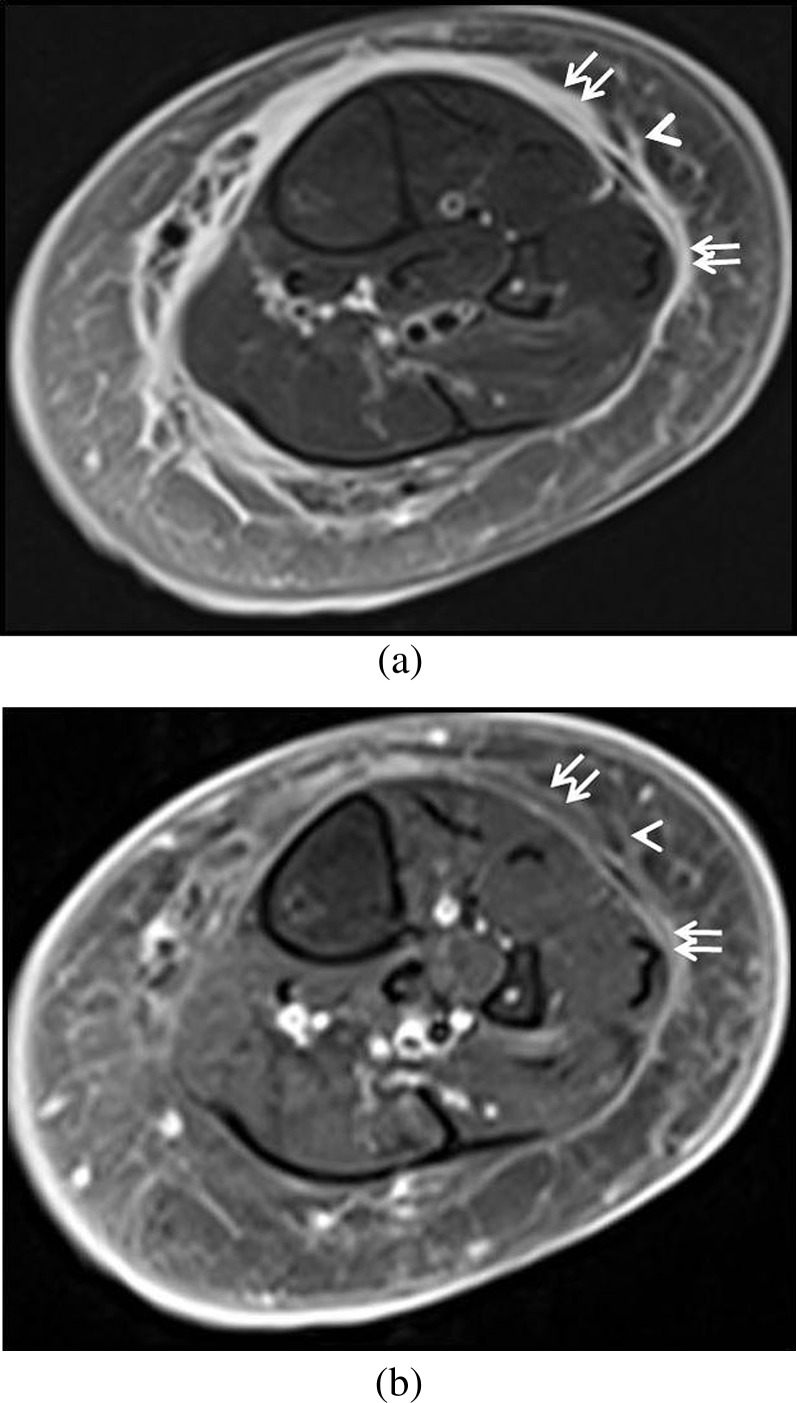
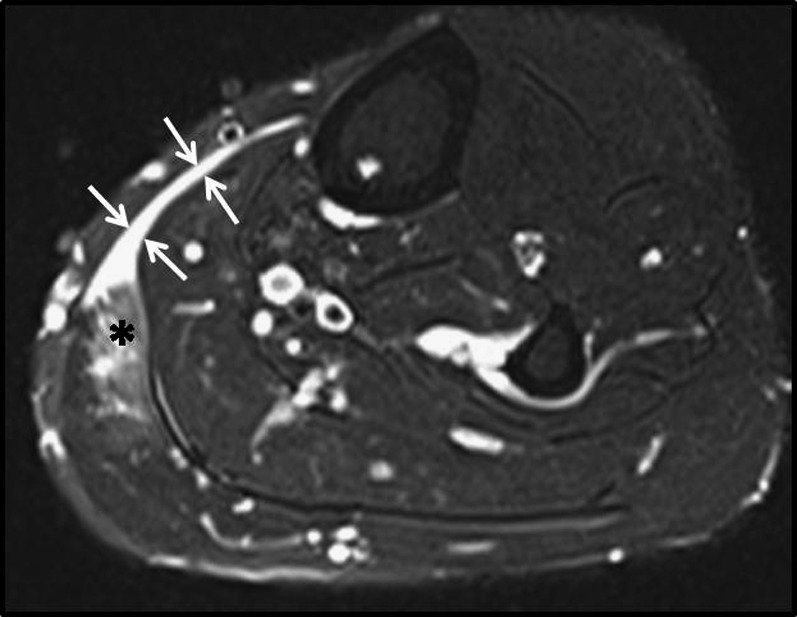
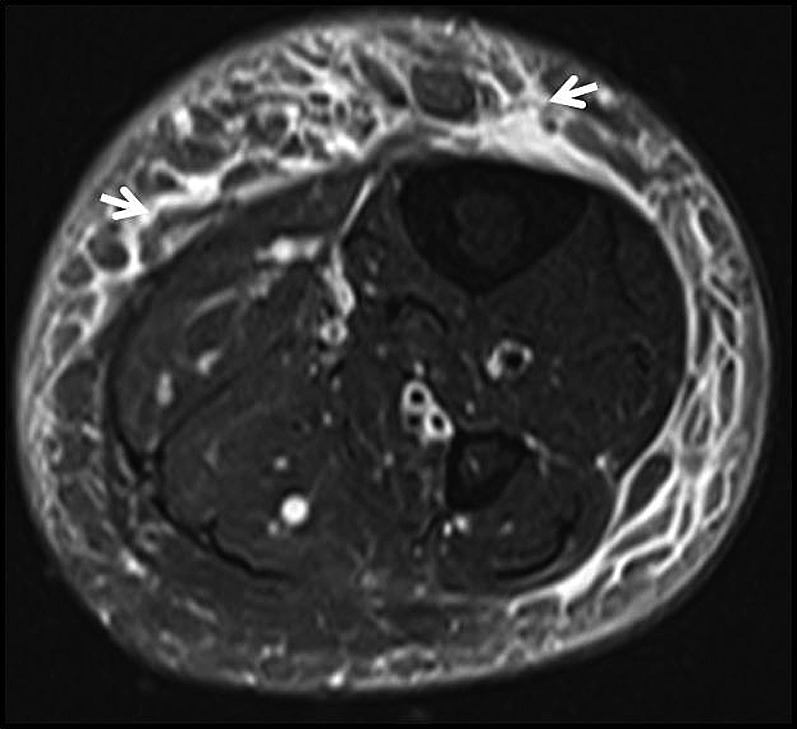
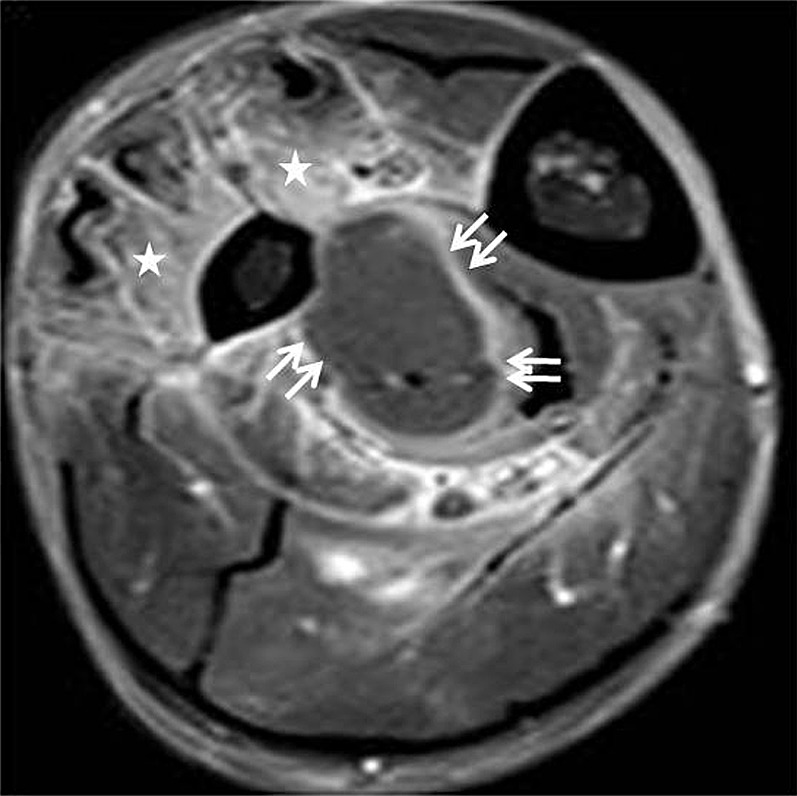
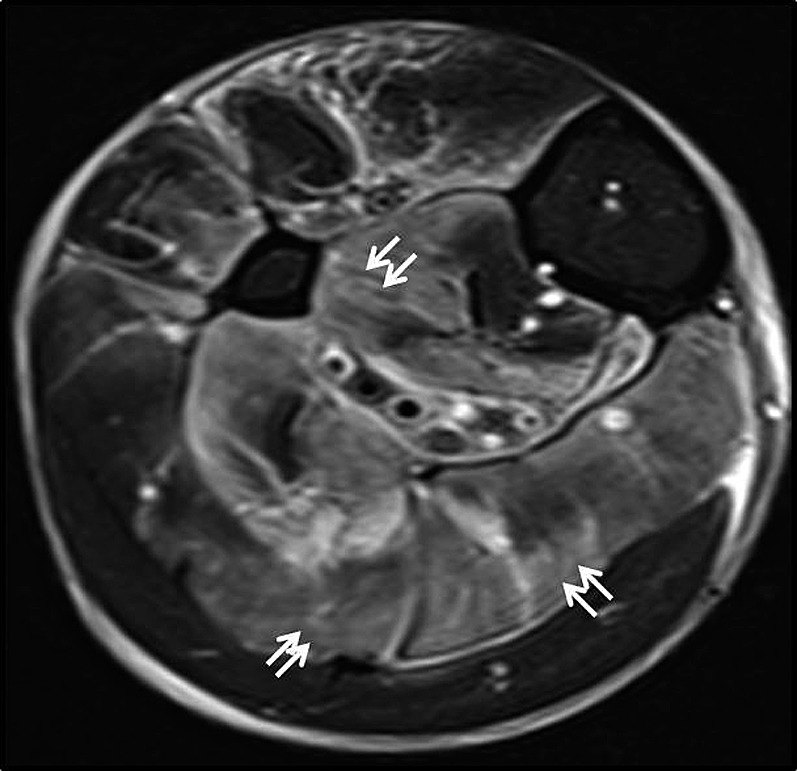
Necrotizing fasciitis is a life-threatening soft-tissue infection of bacterial origin, which involves mainly the deep fascia. Early recognition of this condition may be hampered by the uncommon nature of the disease and non-specificity of initial clinical signs and symptoms in less fulminant cases, making the role of imaging important. MRI is the most useful imaging modality in the diagnosis of necrotizing fasciitis. The presence of thick (>3 mm) hyperintense signal in the deep fascia (particularly intermuscular fascia) on fat-suppressed T2 weighted or short tau inversion-recovery images is an important marker for necrotizing fasciitis. Contrast enhancement of the thickened necrotic fascia can be variable, with a mixed-pattern of enhancement being more commonly encountered. Involvement of multiple musculofascial compartments increases the likelihood of necrotizing fasciitis. It is important to remember that T2-hyperintense signal in the deep fascia is not specific to necrotizing fasciitis and can also be seen in cases such as non-infective inflammatory fasciitis or muscle tear. In this pictorial essay, we aim to review the MRI findings in necrotizing fasciitis, discuss its limitations and pitfalls and identify differentiating features from non-necrotizing soft-tissue infections, such as cellulitis and infective myositis/pyomyositis, conditions which may clinically mimic necrotizing fasciitis.
Figures
Similar articles
-
Can necrotizing infectious fasciitis be differentiated from nonnecrotizing infectious fasciitis with MR imaging?Radiology. 2011 Jun;259(3):816-24. doi: 10.1148/radiol.11101164. Epub 2011 Mar 15. Radiology. 2011. PMID: 21406630
-
Deep fascial hyperintensity in soft-tissue abnormalities as revealed by T2-weighted MR imaging.AJR Am J Roentgenol. 1997 May;168(5):1301-4. doi: 10.2214/ajr.168.5.9129430. AJR Am J Roentgenol. 1997. PMID: 9129430
-
Differentiation of necrotizing fasciitis and cellulitis using MR imaging.AJR Am J Roentgenol. 1998 Mar;170(3):615-20. doi: 10.2214/ajr.170.3.9490940. AJR Am J Roentgenol. 1998. PMID: 9490940
-
Acute swelling of the limbs: magnetic resonance pictorial review of fascial and muscle signal changes.Eur J Radiol. 1999 Apr;30(1):11-21. doi: 10.1016/s0720-048x(98)00119-3. Eur J Radiol. 1999. PMID: 10389007 Review.
-
Necrotizing fasciitis: contribution and limitations of diagnostic imaging.Joint Bone Spine. 2013 Mar;80(2):146-54. doi: 10.1016/j.jbspin.2012.08.009. Epub 2012 Oct 6. Joint Bone Spine. 2013. PMID: 23043899 Review.
Cited by
-
Necrotizing fasciitis following an arthroscopic shoulder surgery: a case report and literature review.JSES Rev Rep Tech. 2023 May 27;3(4):548-552. doi: 10.1016/j.xrrt.2023.04.004. eCollection 2023 Nov. JSES Rev Rep Tech. 2023. PMID: 37928981 Free PMC article. No abstract available.
-
Clinics in diagnostic imaging (179). Severe rhabdomyolysis complicated by myonecrosis.Singapore Med J. 2017 Aug;58(8):467-472. doi: 10.11622/smedj.2017081. Singapore Med J. 2017. PMID: 28848989 Free PMC article.
-
Diagnostic Key Points and Surgical Management of Necrotizing Fasciitis: A Retrospective Study.Int J Low Extrem Wounds. 2024 Mar;23(1):153-160. doi: 10.1177/15347346211045282. Epub 2021 Oct 6. Int J Low Extrem Wounds. 2024. PMID: 34612747 Free PMC article.
-
Imaging of MSK infections in the ER.Skeletal Radiol. 2024 Oct;53(10):2039-2050. doi: 10.1007/s00256-023-04554-7. Epub 2023 Dec 26. Skeletal Radiol. 2024. PMID: 38147081 Review.
-
Triple diagnostics for early detection of ambivalent necrotizing fasciitis.World J Emerg Surg. 2016 Oct 11;11:51. doi: 10.1186/s13017-016-0108-z. eCollection 2016. World J Emerg Surg. 2016. PMID: 27766113 Free PMC article.
References
-
- Brothers TE, Tagge DU, Stutley JE, Conway WF, Del Schutte H Jr, Byrne TK. Magnetic resonance imaging differentiates between necrotizing and non-necrotizing fasciitis of the lower extremity. J Am Coll Surg 1998; 187: 416-21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
