

Immigrant health inequalities in the United States: use of eight major national data systems
- PMID: 24288488
- PMCID: PMC3826317
- DOI: 10.1155/2013/512313
Immigrant health inequalities in the United States: use of eight major national data systems
Abstract
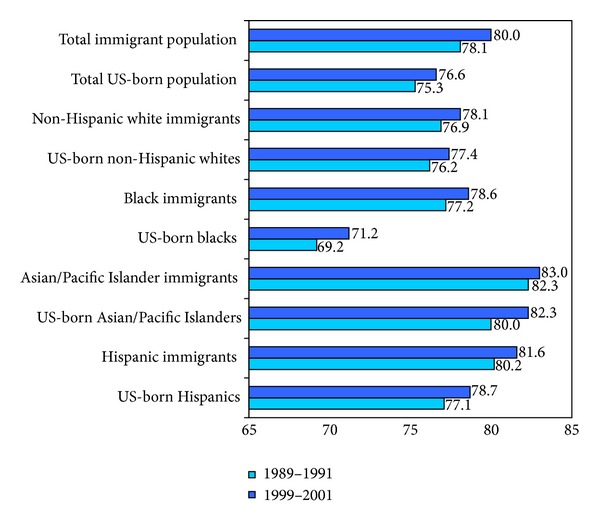
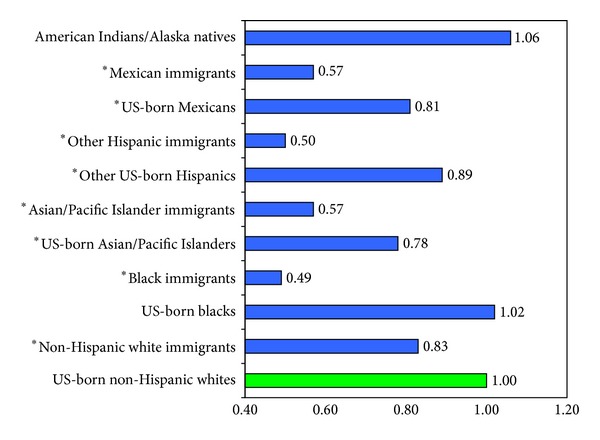
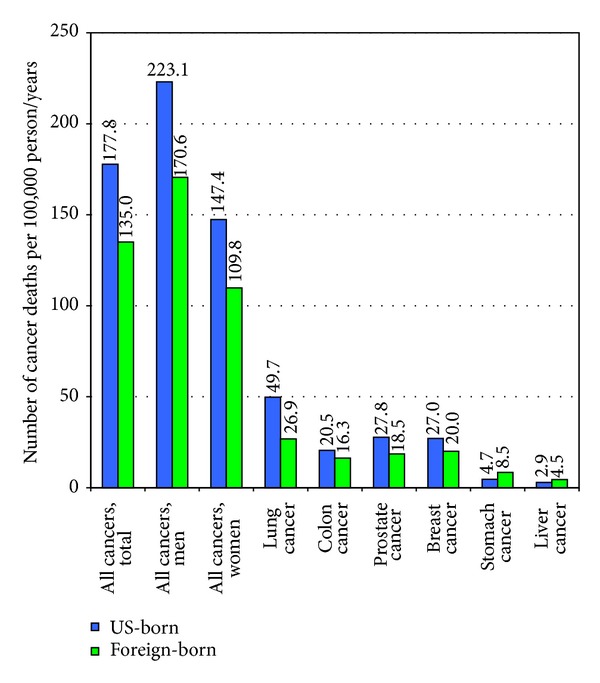
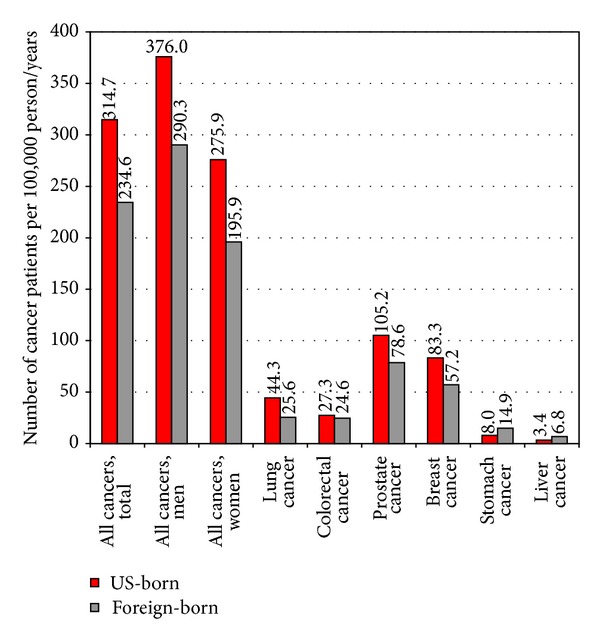
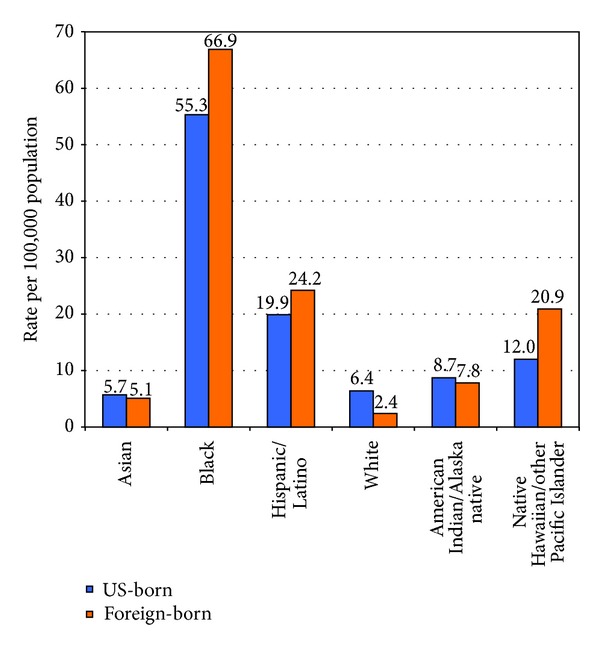
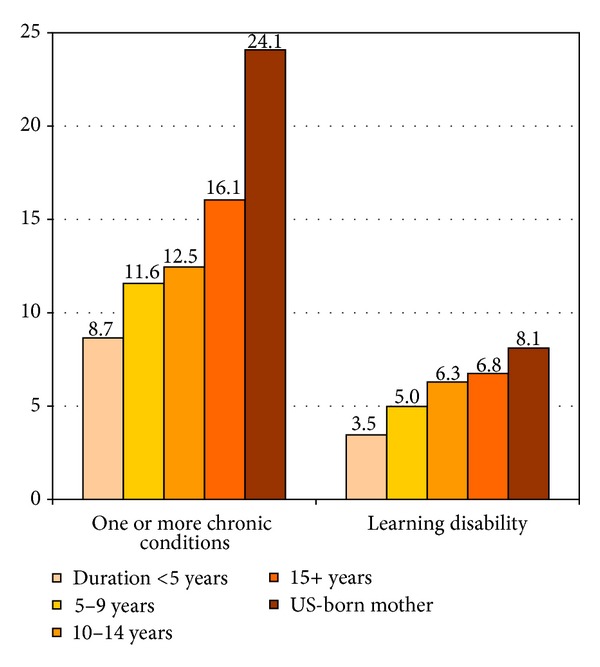
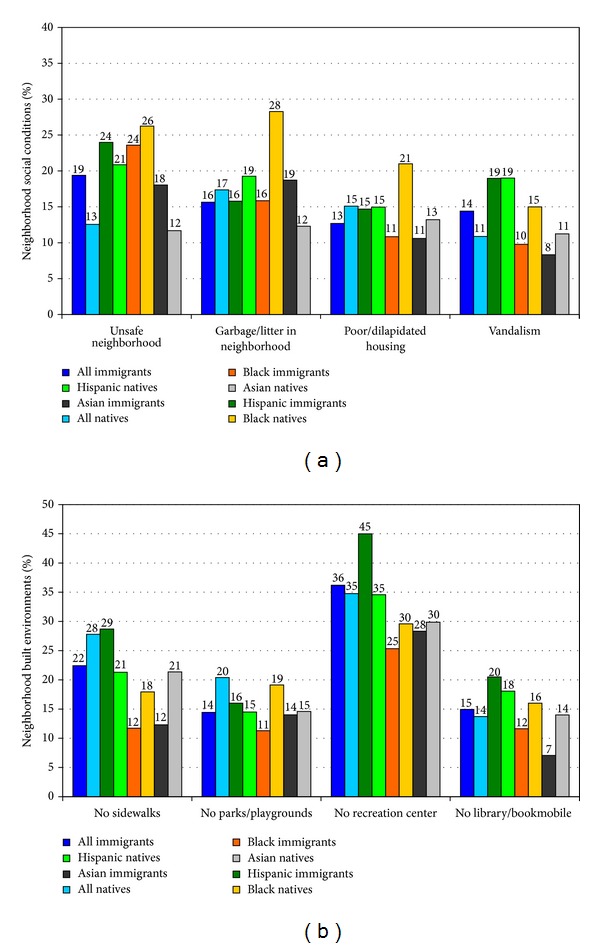
Eight major federal data systems, including the National Vital Statistics System (NVSS), National Health Interview Survey (NHIS), National Survey of Children's Health, National Longitudinal Mortality Study, and American Community Survey, were used to examine health differentials between immigrants and the US-born across the life course. Survival and logistic regression, prevalence, and age-adjusted death rates were used to examine differentials. Although these data systems vary considerably in their coverage of health and behavioral characteristics, ethnic-immigrant groups, and time periods, they all serve as important research databases for understanding the health of US immigrants. The NVSS and NHIS, the two most important data systems, include a wide range of health variables and many racial/ethnic and immigrant groups. Immigrants live 3.4 years longer than the US-born, with a life expectancy ranging from 83.0 years for Asian/Pacific Islander immigrants to 69.2 years for US-born blacks. Overall, immigrants have better infant, child, and adult health and lower disability and mortality rates than the US-born, with immigrant health patterns varying across racial/ethnic groups. Immigrant children and adults, however, fare substantially worse than the US-born in health insurance coverage and access to preventive health services. Suggestions and new directions are offered for improvements in health monitoring and for strengthening and developing databases for immigrant health assessment in the USA.
Figures
References
-
- Walters LP, Trevelyan EN. The Newly Arrived Foreign-Born Population of the United States: 2010. American Community Survey Briefs. Washington, DC, USA: US Census Bureau; 2011.
-
- Grieco EM, Trevelyan EN. Place of Birth of the Foreign-Born Population: 2009. American Community Survey Briefs. Washington, DC, USA: US Census Bureau; 2010.
-
- Grieco EM. Race and Hispanic Origin of the Foreign-Born Population in the United States: 2007. American Community Survey Briefs. Washington, DC, USA: US Census Bureau; 2010.
-
- Larsen LJ. The Foreign-Born Population in the United States: 2003. Current Population Reports, P20-551. Washington, DC, USA: US Census Bureau; 2003.
-
- US Census Bureau. The 2011 American Community Survey. Washington, DC, USA, US Census Bureau, 2012, http://www.census.gov/acs/www/
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
