

Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: a retrospective observational study
- PMID: 24289206
- PMCID: PMC4056656
- DOI: 10.1186/cc13133
Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: a retrospective observational study
Abstract
Introduction: The role of systemic hemodynamics in the pathogenesis of septic acute kidney injury (AKI) has received little attention. The purpose of this study was to investigate the association between systemic hemodynamics and new or persistent of AKI in severe sepsis.
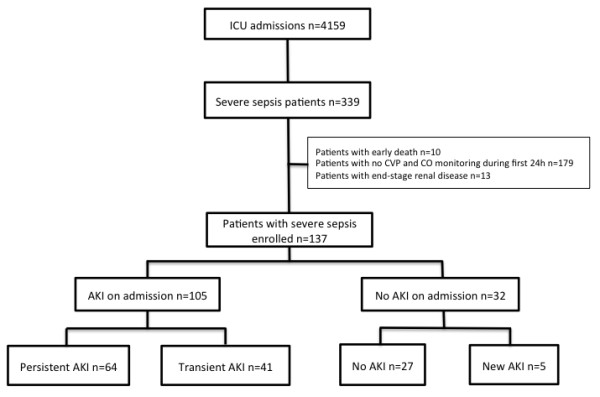
Methods: A retrospective study between 2006 and 2010 was performed in a surgical ICU in a teaching hospital. AKI was defined as development (new AKI) or persistent AKI during the five days following admission based on the Acute Kidney Injury Network (AKIN) criteria. We studied the association between the following hemodynamic targets within 24 hours of admission and AKI: central venous pressure (CVP), cardiac output (CO), mean arterial pressure (MAP), diastolic arterial pressure (DAP), central venous oxygen saturation (ScvO2) or mixed venous oxygen saturation (SvO2).
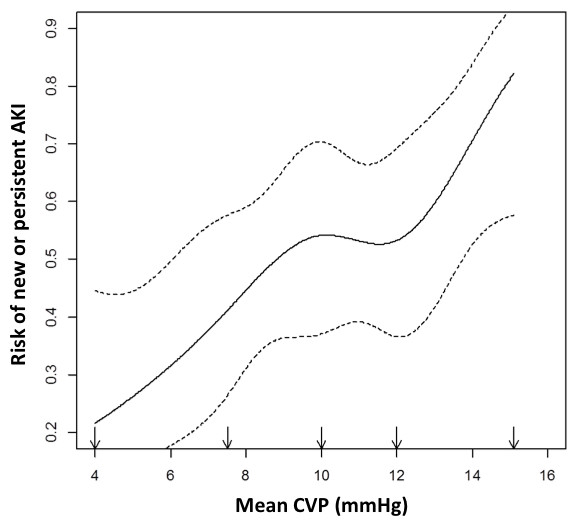
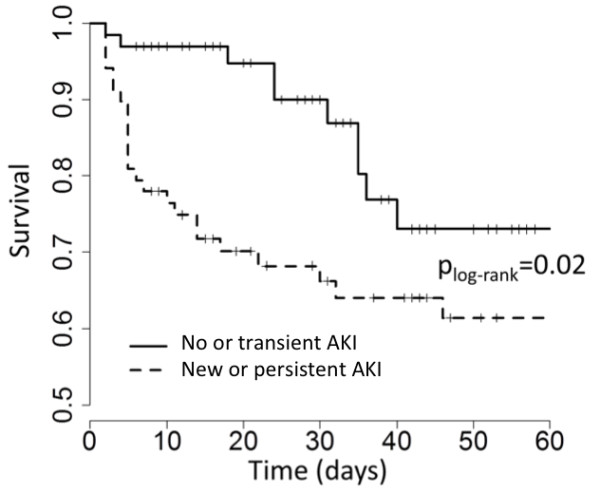
Results: This study included 137 ICU septic patients. Of these, 69 had new or persistent AKI. AKI patients had a higher Simplified Acute Physiology Score (SAPS II) (57 (46 to 67) vs. 45 (33 to 52), P < 0.001) and higher mortality (38% vs. 15%, P = 0.003) than those with no AKI or improving AKI. MAP, ScvO2 and CO were not significantly different between groups. Patients with AKI had lower DAP and higher CVP (P = 0.0003). The CVP value was associated with the risk of developing new or persistent AKI even after adjustment for fluid balance and positive end-expiratory pressure (PEEP) level (OR = 1.22 (1.08 to 1.39), P = 0.002). A linear relationship between CVP and the risk of new or persistent AKI was observed.
Conclusions: We observed no association between most systemic hemodynamic parameters and AKI in septic patients. Association between elevated CVP and AKI suggests a role of venous congestion in the development of AKI. The paradigm that targeting high CVP may reduce occurrence of AKI should probably be revised. Furthermore, DAP should be considered as a potential important hemodynamic target for the kidney.
Figures
Comment in
-
Venous congestion: are we adding insult to kidney injury in sepsis?Crit Care. 2014 Jan 27;18(1):104. doi: 10.1186/cc13709. Crit Care. 2014. PMID: 24467922 Free PMC article.
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;17:813–818. doi: 10.1001/jama.294.7.813. - DOI - PubMed
-
- Payen D, Lukaszewicz AC, Legrand M, Gayat E, Faivre V, Megarbane B, Azoulay E, Fieux F, Charron D, Loiseau P, Busson M. A multicentre study of acute kidney injury in severe sepsis and septic shock: association with inflammatory phenotype and HLA genotype. PLoS ONE. 2012;17:e35838. doi: 10.1371/journal.pone.0035838. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
