

Mortality in rheumatoid arthritis: the impact of disease activity, treatment with glucocorticoids, TNFα inhibitors and rituximab
- PMID: 24291654
- PMCID: PMC4316844
- DOI: 10.1136/annrheumdis-2013-204021
Mortality in rheumatoid arthritis: the impact of disease activity, treatment with glucocorticoids, TNFα inhibitors and rituximab
Abstract
Objectives: To investigate the impact of disease activity, the course of the disease, its treatment over time, comorbidities and traditional risk factors on survival.
Methods: Data of the German biologics register RABBIT were used. Cox regression was applied to investigate the impact of time-varying covariates (disease activity as measured by the DAS28, functional capacity, treatment with glucocorticoids, biologic or synthetic disease modifying antirheumatic drugs (DMARDs)) on mortality after adjustment for age, sex, comorbid conditions and smoking.
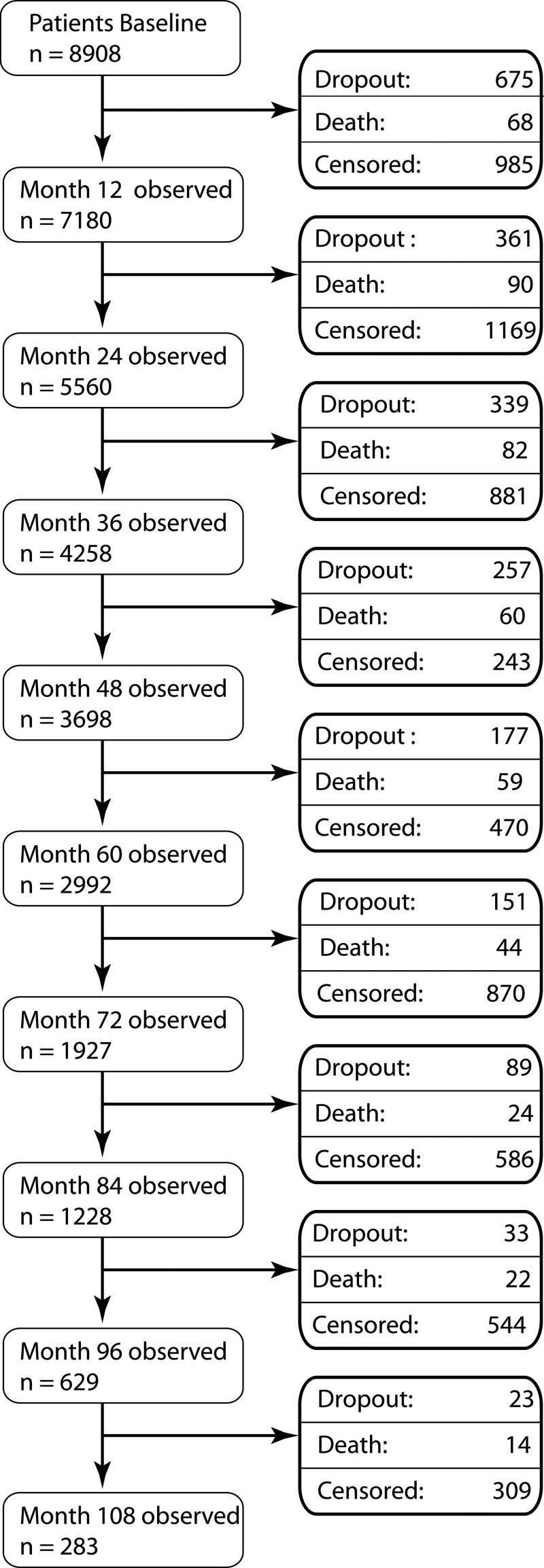
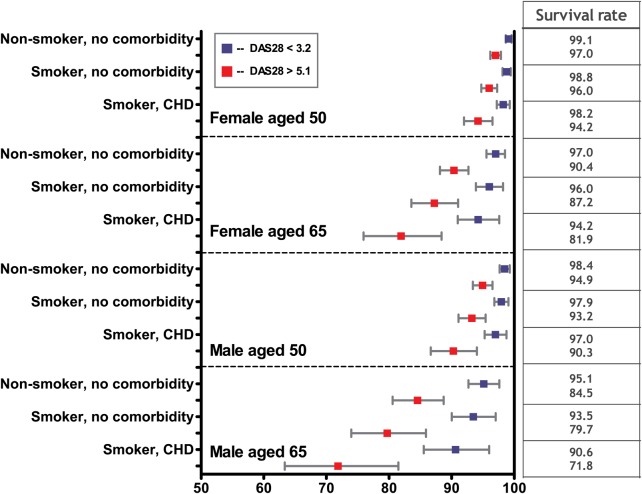
Results: During 31 378 patient-years of follow-up, 463 of 8908 patients died (standardised mortality ratio: 1.49 (95% CI 1.36 to 1.63)). Patients with persistent, highly active disease (mean DAS28 > 5.1) had a significantly higher mortality risk (adjusted HR (HRadj)=2.43; (95% CI 1.64 to 3.61)) than patients with persistently low disease activity (mean DAS28 < 3.2). Poor function and treatment with glucocorticoids > 5 mg/d was significantly associated with an increased mortality, independent of disease activity. Significantly lower mortality was observed in patients treated with tumour necrosis factor α (TNFα) inhibitors (HRadj=0.64 (95% CI 0.50 to 0.81), rituximab (HRadj=0.57 (95% CI 0.39 to 0.84), or other biologics (HRadj=0.64 (95% CI 0.42 to 0.99), compared to those receiving methotrexate. To account for treatment termination in patients at risk, an HRadj for patients ever exposed to TNFα inhibitors or rituximab was calculated. This resulted in an HRadj of 0.77 (95% CI 0.60 to 0.97).
Conclusions: Patients with long-standing high disease activity are at substantially increased risk of mortality. Effective control of disease activity decreases mortality. TNFα inhibitors and rituximab seem to be superior to conventional DMARDs in reducing this risk.
Keywords: DAS28; DMARDs (biologic); Methotrexate; Rheumatoid Arthritis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Cobb S, Anderson F, Bauer W. Length of life and cause of death in rheumatoid arthritis. N Engl J Med 1953;249:553–6. - PubMed
-
- Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum 1994;37:481–94. - PubMed
-
- Bjornadal L, Baecklund E, Yin L, et al. Decreasing mortality in patients with rheumatoid arthritis: results from a large population based cohort in Sweden, 1964–95. J Rheumatol 2002;29:906–12. - PubMed
-
- Gonzalez A, Maradit KH, Crowson CS, et al. The widening mortality gap between rheumatoid arthritis patients and the general population. Arthritis Rheum 2007;56:3583–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
