

Modification of the association between obesity and lethal prostate cancer by TMPRSS2:ERG
- PMID: 24292212
- PMCID: PMC3866157
- DOI: 10.1093/jnci/djt332
Modification of the association between obesity and lethal prostate cancer by TMPRSS2:ERG
Abstract
Background: TMPRSS2:ERG is a hormonally regulated gene fusion present in about half of prostate tumors. We investigated whether obesity, which deregulates several hormonal pathways, interacts with TMPRSS2:ERG to impact prostate cancer outcomes.
Methods: The study included 1243 participants in the prospective Physicians' Health Study and Health Professionals Follow-Up Study diagnosed with prostate cancer between 1982 and 2005. ERG overexpression (a TMPRSS2:ERG marker) was assessed by immunohistochemistry of tumor tissue from radical prostatectomy or transurethral resection of the prostate. Body mass index (BMI) and waist circumference, measured on average 1.3 years and 5.3 years before diagnosis, respectively, were available from questionnaires. Data on BMI at baseline was also available. We used Cox regression to calculate hazard ratios and 95% confidence intervals (CIs). All statistical tests were two-sided.
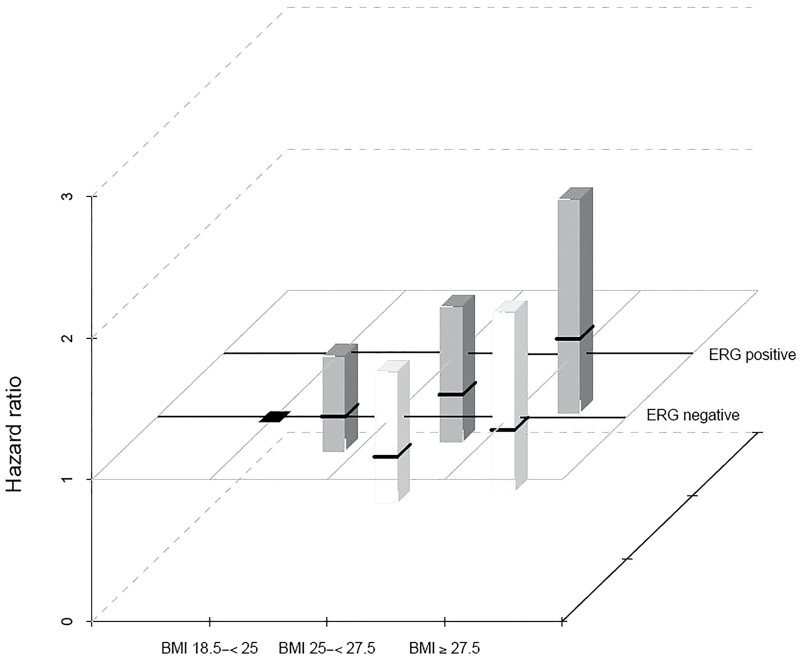
Results: During a mean follow-up of 12.8 years, 119 men developed lethal disease (distant metastases or prostate cancer death). Among men with ERG-positive tumors, the multivariable hazard ratio for lethal prostate cancer was 1.48 (95% CI = 0.98 to 2.23) per 5-unit increase in BMI before diagnosis, 2.51 (95% CI = 1.26 to 4.99) per 8-inch increase in waist circumference before diagnosis, and 2.22 (95% CI = 1.35 to 3.63) per 5-unit increase in BMI at baseline. The corresponding hazard ratios among men with ERG-negative tumors were 1.10 (95% CI = 0.76 to1.59; P interaction = .24), 1.14 (95% CI = 0.62 to 2.10; P interaction = .09), and 0.78 (95% CI = 0.52 to 1.19; P interaction = .001).
Conclusions: These results suggest that obesity is linked with poorer prostate cancer prognosis primarily in men with tumors harboring the gene fusion TMPRSS2:ERG.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2013. Atlanta, GA: American Cancer Society; 2013.
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303(3):235–241 - PubMed
-
- Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–591 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA-40360/CA/NCI NIH HHS/United States
- CA-34944/CA/NCI NIH HHS/United States
- P50 CA090381/CA/NCI NIH HHS/United States
- HL-34595/HL/NHLBI NIH HHS/United States
- HL-26490/HL/NHLBI NIH HHS/United States
- P01 CA055075/CA/NCI NIH HHS/United States
- CA55075/CA/NCI NIH HHS/United States
- 5P50CA090381-08/CA/NCI NIH HHS/United States
- R01 HL026490/HL/NHLBI NIH HHS/United States
- T32 CA009001/CA/NCI NIH HHS/United States
- CA-097193/CA/NCI NIH HHS/United States
- R01 CA097193/CA/NCI NIH HHS/United States
- CA141298/CA/NCI NIH HHS/United States
- R01 HL034595/HL/NHLBI NIH HHS/United States
- U01 CA113913/CA/NCI NIH HHS/United States
- R25 CA098566/CA/NCI NIH HHS/United States
- R01 CA040360/CA/NCI NIH HHS/United States
- R01 CA136578/CA/NCI NIH HHS/United States
- R01 CA034944/CA/NCI NIH HHS/United States
- CA13389/CA/NCI NIH HHS/United States
- R01 CA141298/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
