

IL-2 therapy promotes suppressive ICOS+ Treg expansion in melanoma patients
- PMID: 24292706
- PMCID: PMC3871216
- DOI: 10.1172/JCI46266
IL-2 therapy promotes suppressive ICOS+ Treg expansion in melanoma patients
Abstract
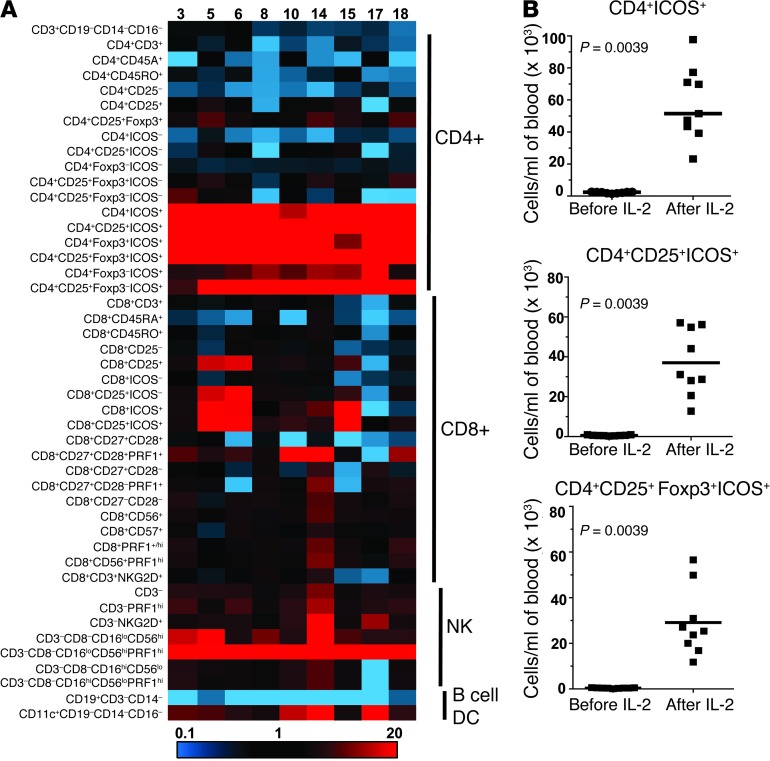
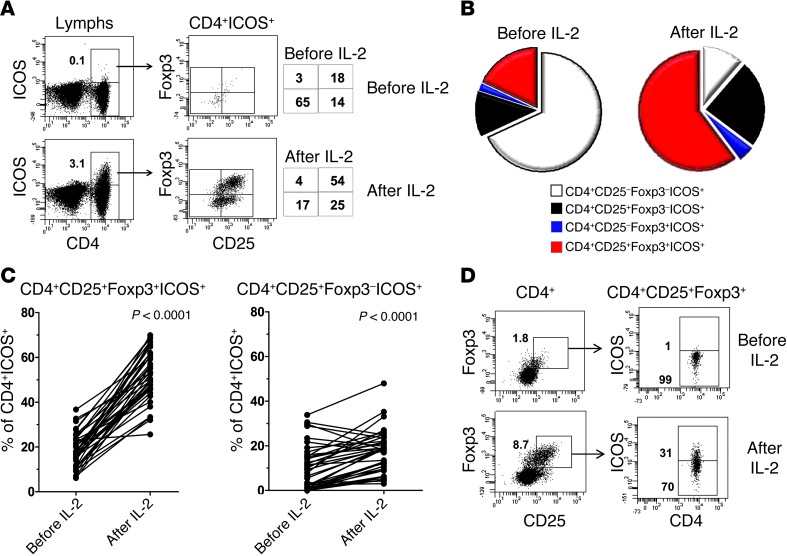
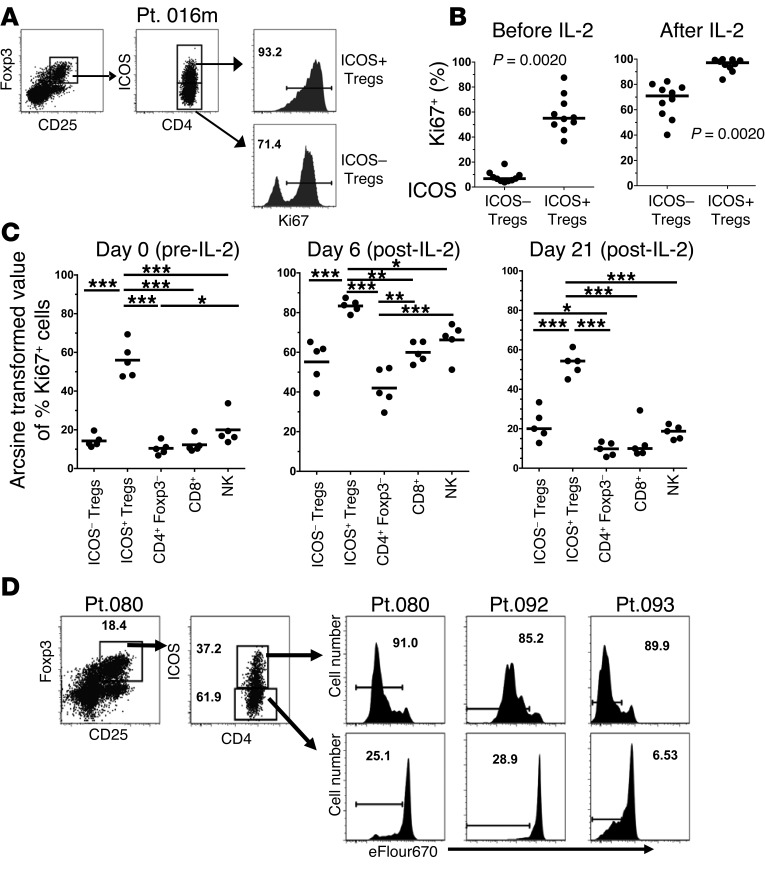
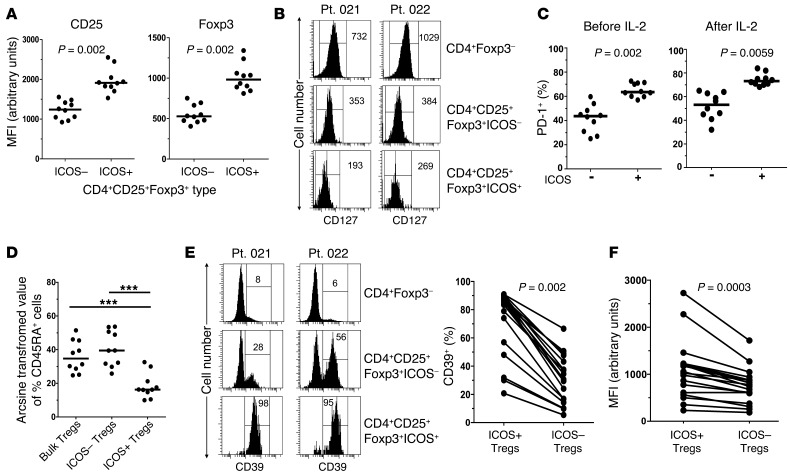
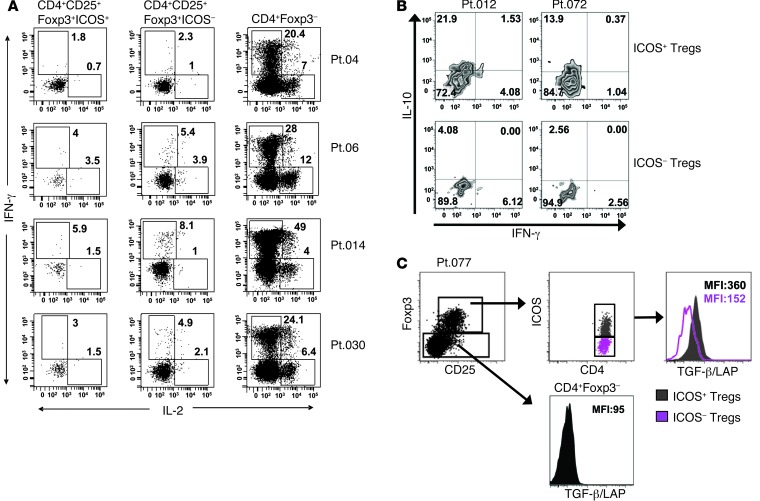
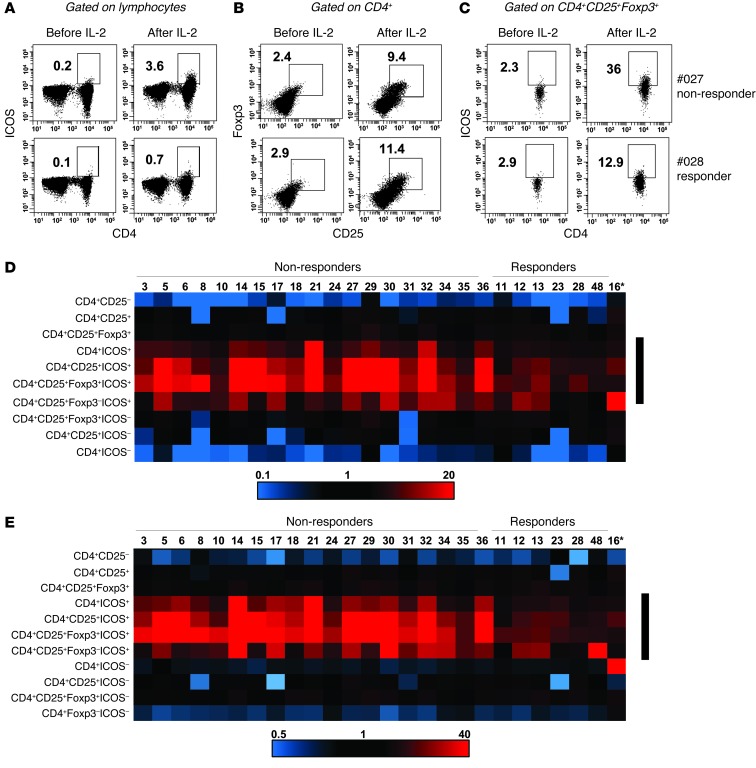
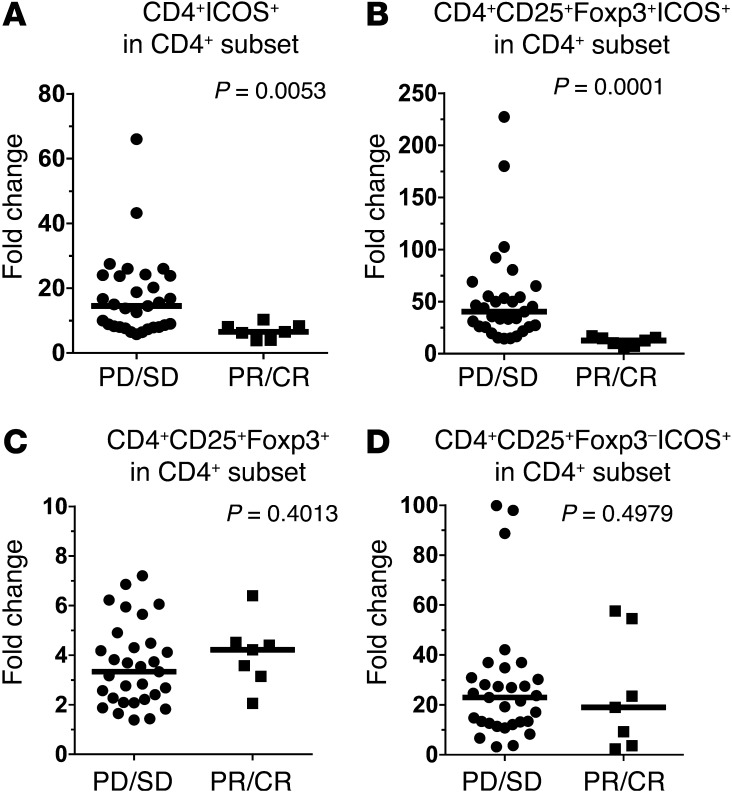
High-dose (HD) IL-2 therapy in patients with cancer increases the general population of Tregs, which are positive for CD4, CD25, and the Treg-specific marker Foxp3. It is unknown whether specific subsets of Tregs are activated and expanded during HD IL-2 therapy or whether activation of any particular Treg subset correlates with clinical outcome. Here, we evaluated Treg population subsets that were induced in patients with melanoma following HD IL-2 therapy. We identified a Treg population that was positive for CD4, CD25, Foxp3, and the inducible T cell costimulator (ICOS). This Treg population increased more than any other lymphocyte subset during HD IL-2 therapy and had an activated Treg phenotype, as indicated by high levels of CD39, CD73, and TGF-β. ICOS(+) Tregs were the most proliferative lymphocyte population in the blood after IL-2 therapy. Patients with melanoma with enhanced expansion of ICOS(+) Tregs in blood following the first cycle of HD IL-2 therapy had worse clinical outcomes than patients with fewer ICOS(+) Tregs. However, there was no difference in total Treg expansion between HD IL-2 responders and nonresponders. These data suggest that increased expansion of the ICOS(+) Treg population following the first cycle of HD IL-2 therapy may be predictive of clinical outcome.
Figures
References
-
- Atkins MB, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993. J Clin Oncol. 1999;17(7):2105–2116. - PubMed
-
- Dutcher J. Current status of interleukin-2 therapy for metastatic renal cell carcinoma and metastatic melanoma. Oncology (Williston Park). 2002;16(11 suppl 13):4–10. - PubMed
-
- Fyfe G, et al. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol. 1995;13(3):688–696. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
