

Atypical ultrasound features of parathyroid tumours may bear a relationship to their clinical and biochemical presentation
- PMID: 24293304
- PMCID: PMC3948912
- DOI: 10.1007/s13244-013-0297-x
Atypical ultrasound features of parathyroid tumours may bear a relationship to their clinical and biochemical presentation
Abstract
Objectives: To describe atypical ultrasound features of parathyroid lesions and correlate them with clinical presentation and histopathology.
Materials and methods: Retrospective review of 264 patients with primary hyperparathyroidism who underwent ultrasound imaging prior to parathyroidectomy was performed. Patients with atypical ultrasound findings (n = 26) were identified; imaging findings were correlated with clinical presentation and histopathology.
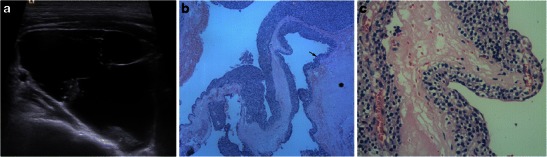
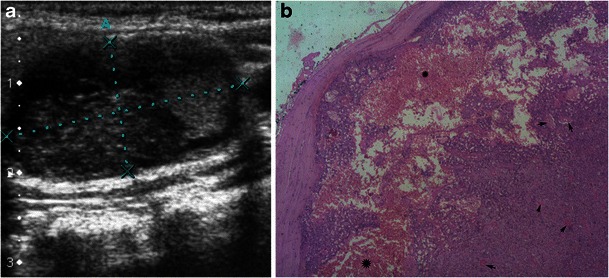
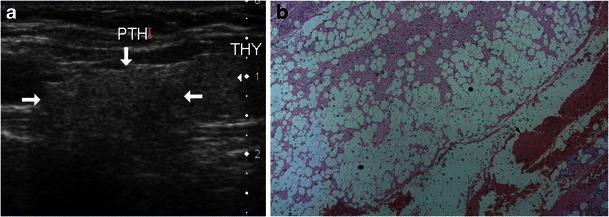
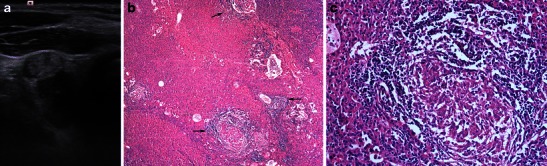
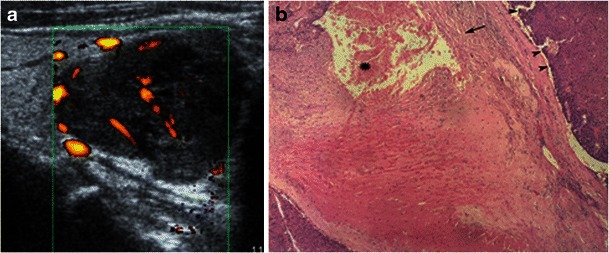
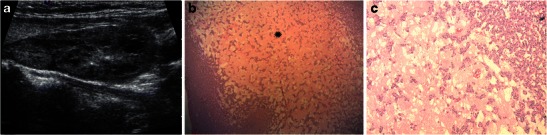
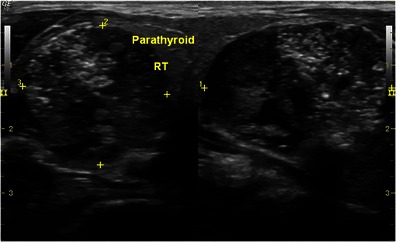
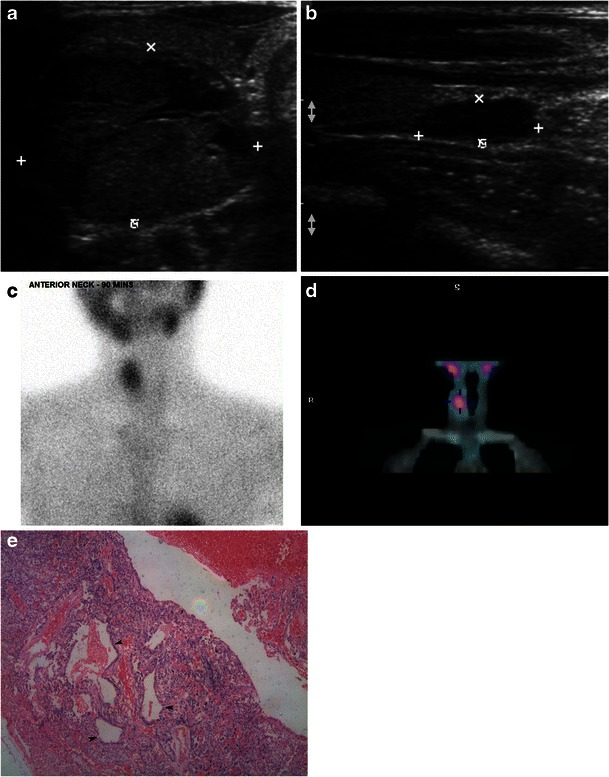
Results: Twenty-one (80 %) lesions were adenomas, two (8 %) were adenomas with cellular atypia, and three (11.5 %) were carcinomas. Seventeen (65 %) lesions showed cystic change; five (19 %) of them had >50 % cystic change. These lesions were adenomas with cystic degeneration. Cystic degeneration had significant positive correlation with the lesion size and PTH level, but cystic adenomas correlated negatively with lesion weight. Six (23 %) lesions were isoechoic and one (4 %) was hyperechoic; histology predominantly revealed haemorrhage, hyalinisation and fibrosis; one lesion showed fat deposition and another had multiple granulomas within the adenoma. Twenty (83 %) lesions had heterogeneous echotexture and showed combinations of acinar dilatation, necrosis, haemorrhage and fibrosis. Heterogeneous lesions tended to be significantly larger and heavier, and they were associated with higher PTH levels. Four (15 %) lesions had calcifications. Scintigraphy was concordant in 22 (96 %), n = 23. One scintigraphy-negative lesion was a cystic parathyroid adenoma.
Conclusion: Atypical ultrasound features of parathyroid lesions pose a diagnostic challenge. Awareness of these features would help improve lesion detection.
Teaching points: 1. Cystic change is significantly related to the size, weight and measured parathyroid hormone levels. 2. Cystic change in parathyroid tumours indicated a slightly higher risk of malignancy. 3. Heterogeneous parathyroid adenomas are larger in size and heavier, and they have higher PTH levels. 4. Awareness of atypical ultrasound features will improve preoperative clinical prediction.
Figures
Similar articles
-
Primary hyperparathyroidism due to atypical vertically long cystic adenoma.Endocrinol Diabetes Metab Case Rep. 2014;2014:140086. doi: 10.1530/EDM-14-0086. Epub 2014 Oct 1. Endocrinol Diabetes Metab Case Rep. 2014. PMID: 25379182 Free PMC article.
-
[18F]Fluorocholine Uptake of Parathyroid Adenoma Is Correlated with Parathyroid Hormone Level.Mol Imaging Biol. 2018 Oct;20(5):857-867. doi: 10.1007/s11307-018-1179-x. Mol Imaging Biol. 2018. PMID: 29508264
-
Cystic Parathyroid Adenomas: An Enigmatic Entity and Role of Tc-99 m Sestamibi Scintigraphy.Endocr Pract. 2021 Jun;27(6):614-620. doi: 10.1016/j.eprac.2020.11.010. Epub 2020 Dec 13. Endocr Pract. 2021. PMID: 34120702
-
Giant parathyroid tumours in primary hyperparathyroidism: a systematic review.Langenbecks Arch Surg. 2022 Mar;407(2):501-516. doi: 10.1007/s00423-021-02406-3. Epub 2022 Jan 18. Langenbecks Arch Surg. 2022. PMID: 35039921
-
Giant cystic parathyroid adenoma: two case reports and a literature review.J Int Med Res. 2022 Jun;50(6):3000605221106419. doi: 10.1177/03000605221106419. J Int Med Res. 2022. PMID: 35734999 Free PMC article. Review.
Cited by
-
Overview of the 2022 WHO Classification of Parathyroid Tumors.Endocr Pathol. 2022 Mar;33(1):64-89. doi: 10.1007/s12022-022-09709-1. Epub 2022 Feb 17. Endocr Pathol. 2022. PMID: 35175514 Review.
-
Evaluation of preoperative ultrasonographic and biochemical features of patients with aggressive parathyroid disease: is there a reliable predictive marker?Arch Endocrinol Metab. 2016 Nov-Dec;60(6):537-544. doi: 10.1590/2359-3997000000224. Epub 2016 Nov 24. Arch Endocrinol Metab. 2016. PMID: 27901181 Free PMC article.
-
Primary hyperparathyroidism-related giant parathyroid adenoma (Review).Exp Ther Med. 2022 Jan;23(1):88. doi: 10.3892/etm.2021.11011. Epub 2021 Nov 26. Exp Ther Med. 2022. PMID: 34934453 Free PMC article. Review.
-
Multimodality Imaging in Patients with Secondary Hypertension: With a Focus on Appropriate Imaging Approaches Depending on the Etiologies.Korean J Radiol. 2018 Mar-Apr;19(2):272-283. doi: 10.3348/kjr.2018.19.2.272. Epub 2018 Feb 22. Korean J Radiol. 2018. PMID: 29520185 Free PMC article.
-
Multi-modality parathyroid imaging: A shifting paradigm.World J Radiol. 2023 Mar 28;15(3):69-82. doi: 10.4329/wjr.v15.i3.69. World J Radiol. 2023. PMID: 37035829 Free PMC article. Review.
References
-
- Reeder SB, Desser TS, Weigel RJ, Jeffrey RB. Sonography in primary hyperparathyroidism: review with emphasis on scanning technique. J Ultrasound Med. 2002;21(5):539–52. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
