

Effectiveness of three sleep apnea management alternatives
- PMID: 24293754
- PMCID: PMC3825429
- DOI: 10.5665/sleep.3204
Effectiveness of three sleep apnea management alternatives
Abstract
Rationale: Home respiratory polygraphy (HRP) may be a cost-effective alternative to polysomnography (PSG) for diagnosis and treatment election in patients with high clinical probability of obstructive sleep apnea (OSA), but there is conflicting evidence on its use for a wider spectrum of patients.
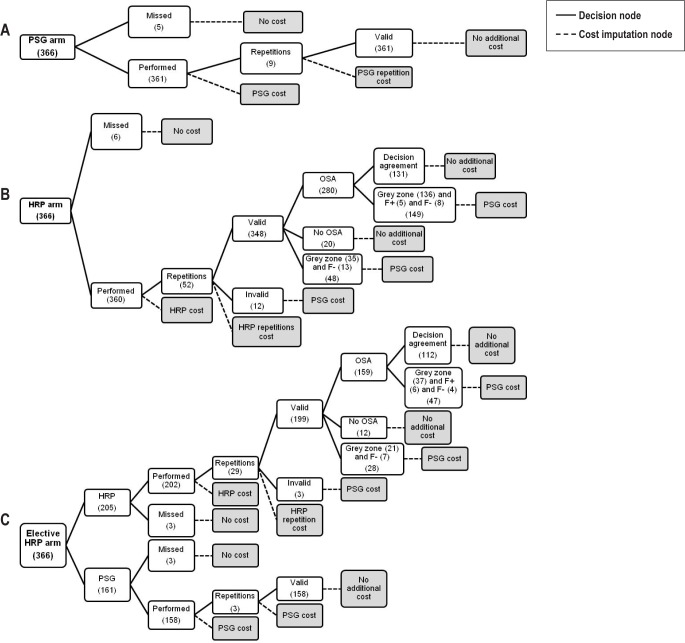
Objectives: To determine the efficacy and cost of OSA management (diagnosis and therapeutic decision making) using (1) PSG for all patients (PSG arm); (2) HRP for all patients (HRP arm); and (3) HRP for a subsample of patients with high clinical probability of being treated with continuous positive airway pressure (CPAP) and PSG for the remainder (elective HRP arm).
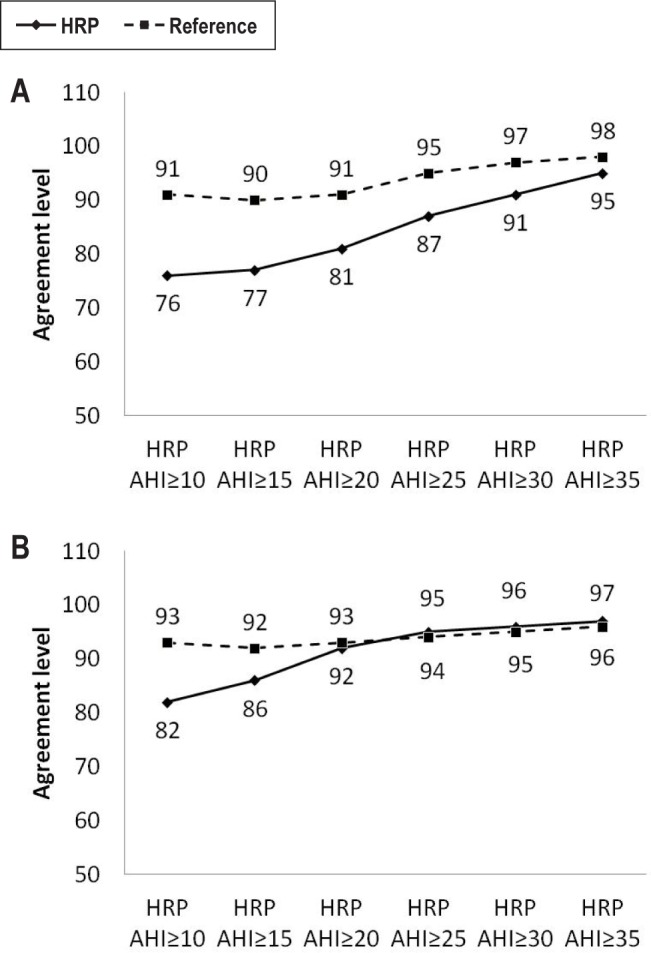
Methods: Multicentric study of 366 patients with intermediate-high clinical probability of OSA, randomly subjected to HRP and PSG. We explored the diagnostic and therapeutic decision agreements between the PSG and both HRP arms for several HRP cutoff points and calculated costs for equal diagnostic and/or therapeutic decision efficacy.
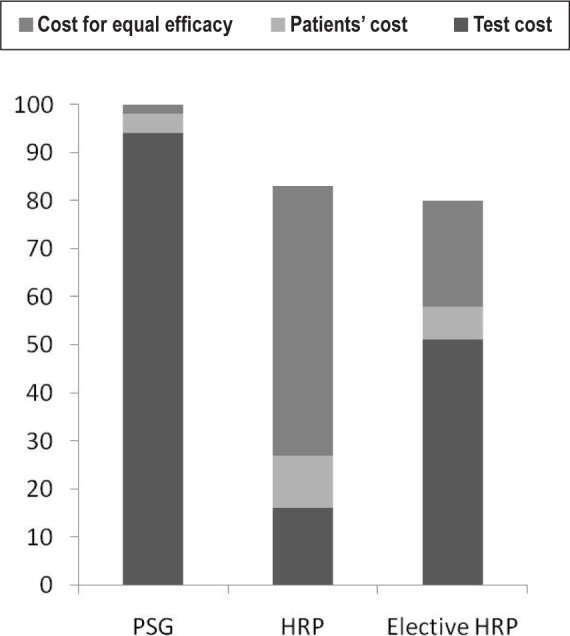
Results: For equal diagnostic and therapeutic decision efficacy, PSG arm costs were 18% higher than HRP arm costs and 20% higher than elective HRP arm costs. HRP arm costs tended to be lower than elective HRP arm costs, and both tended to be lower than PSG arm costs if patient costs were omitted.
Conclusion: Home respiratory polygraphy is a less costly alternative than polysomnography for the diagnosis and therapeutic decision making for patients with suspected obstructive sleep apnea. We found no advantage in cost terms, however, in using home respiratory polygraphy for all patients or home respiratory polygraphy for the most symptomatic patients and polysomnography for the rest.
Keywords: Cost efficacy; home respiratory polygraphy; portable monitor; sleep apnea.
Figures
References
-
- Durán J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163:685–9. - PubMed
-
- Ballester E, Badia JR, Hernández L, et al. Evidence of the effectiveness of continuous positive airway pressure in the treatment of sleep apnea/ hypopnea syndrome. Am J Respir Crit Care Med. 1999;159:495–501. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
-
- Barbé F, Durán-Cantolla J, Sánchez-de-la-Torre M, et al. Spanish Sleep And Breathing Network. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307:2161–8. - PubMed
-
- Terán-Santos J, Jiménez-Gómez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N Engl J Med. 1999;340:847–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
