

Review
doi: 10.1055/s-0032-1330058.
Chest drainage
Affiliations
- PMID: 24293797
- PMCID: PMC3577621
- DOI: 10.1055/s-0032-1330058
Item in Clipboard
Review
Chest drainage
Semin Intervent Radiol.
2012 Dec.
Abstract
Infectious, traumatic, or neoplastic processes in the chest often result in fluid collections within the pleural, parenchymal, or mediastinal spaces. The same fundamental principles that guide drainages of the abdomen can be applied to the chest. This review discusses various pathologic conditions of the thorax that can result in the abnormal accumulation of fluid or air, and their management using image-guided methods.
Keywords: abscess; empyema; pleural effusion; pneumothorax; thoracentesis; thoracostomy.
Figures
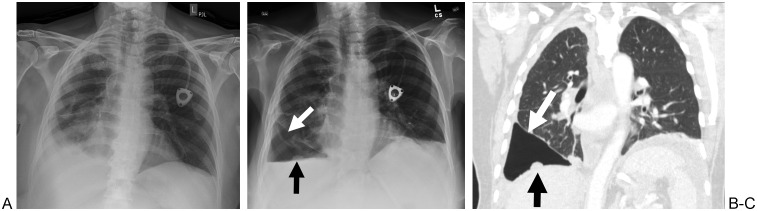
A 65-year-old woman with metastatic ovarian cancer. (A) Frontal radiograph of the chest demonstrates a right pleural effusion. (B) Frontal radiograph of the chest demonstrates a new right hydropneumothorax immediately after right thoracentesis (white arrow). A pleural-based nodule is also noted (black arrow). (C) Coronal computed tomography scan of the chest obtained 1 day after the thoracentesis demonstrates incomplete expansion of the right lower lobe (white arrow), consistent with so-called vacu-thorax. Again demonstrated is the pleural-based metastasis (black arrow). The patient remained asymptomatic throughout her clinical course and did not have any further intervention.
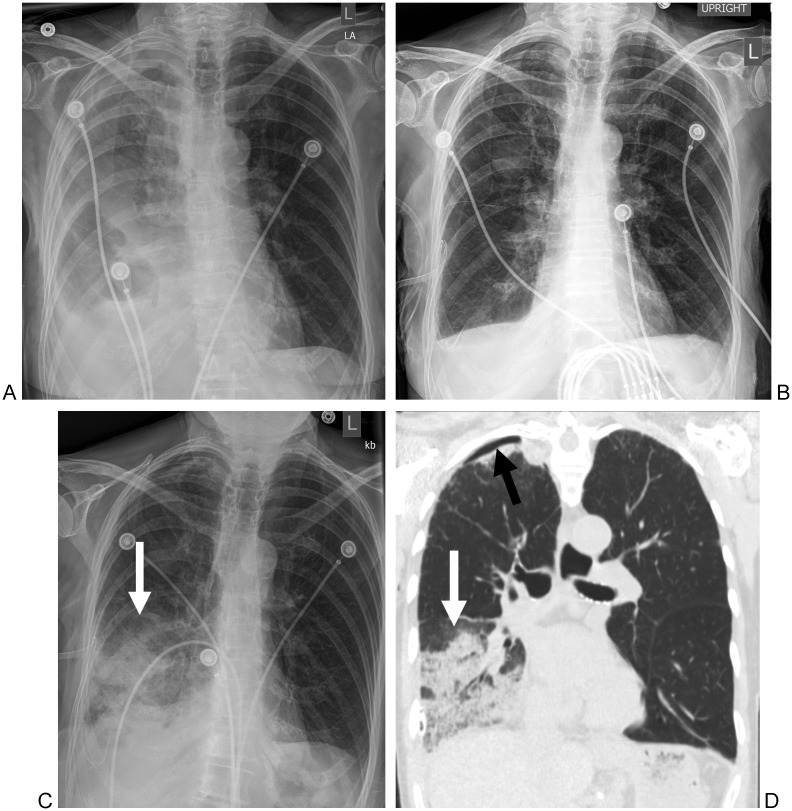
An 88-year-old woman with a history of a recent myocardial infarction. (A) Frontal radiograph of the chest demonstrates a right pleural effusion. (B) Frontal radiograph of the chest immediately after chest drainage shows resolution of the right pleural effusion. (C) Frontal radiograph of the chest obtained 5 hours after chest drainage and obtained for new shortness of breath demonstrates new right lower lobe airspace opacities (arrow). (D) Coronal computed tomography scan of the chest demonstrates right lower lobe airspace disease (white arrow) consistent with reexpansion pulmonary edema. There is also a small right apical pneumothorax (black arrow).
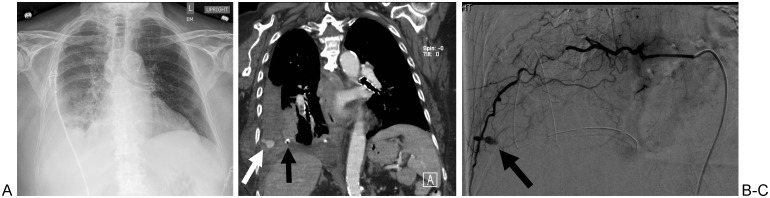
A 68-year-old woman with end-stage renal disease. (A) Frontal radiograph of the chest demonstrates a large right pleural effusion prior to thoracentesis. (B) Coronal computed tomography of the chest demonstrates a pseudoaneurysm of a right intercostal artery (white arrow), adjacent to a drainage catheter (black arrow) that was inserted because of shortness of breath post thoracentesis. (C) Digital subtraction angiogram demonstrates a pseudoaneurysm of a right intercostal artery (black arrow), which was successfully embolized with coils.
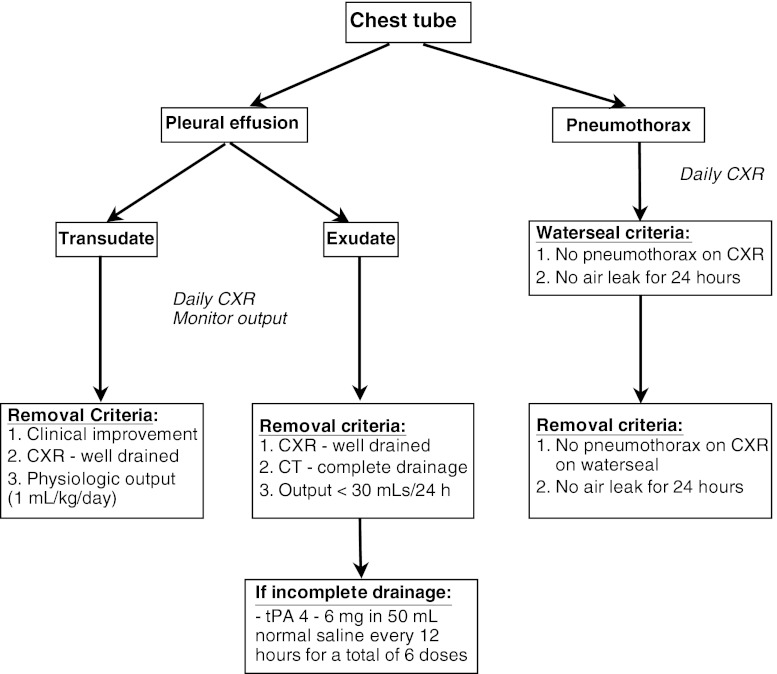
An algorithm for the management of chest tubes. CXR, chest X-ray; tPA, tissue plasminogen activator.
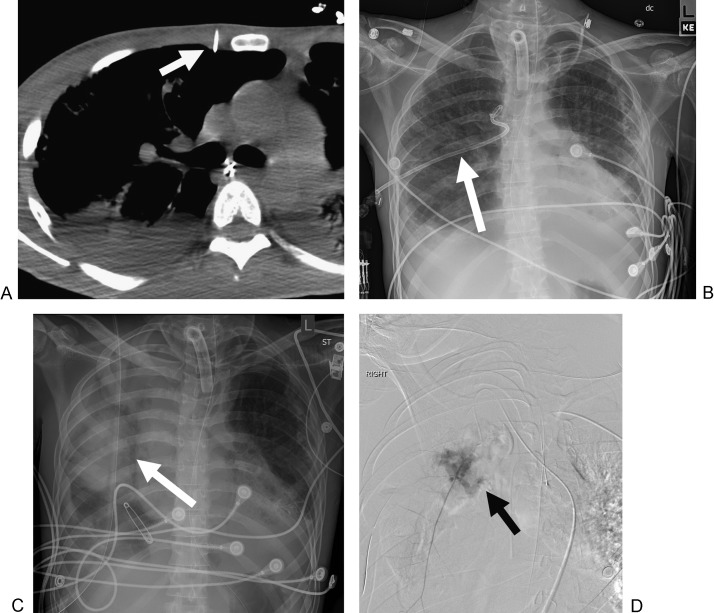
A 23-year-old man with bilateral pneumothoraces secondary to interstitial lung disease. (A) Axial computed tomography image of the chest at the time of the right thoracostomy demonstrates the trajectory of the drainage catheter, immediately adjacent to the internal mammary artery (arrow). (B) Frontal radiograph of the chest prior to the removal of the chest drain (arrow). (C) Frontal radiograph of the chest obtained immediately after right chest drain removal, demonstrating new right airspace and mediastinal (arrow) opacities. (D) Digital subtraction angiogram of the right internal mammary artery demonstrates active extravasation of contrast (arrow). The vessel was successfully embolized with coils.
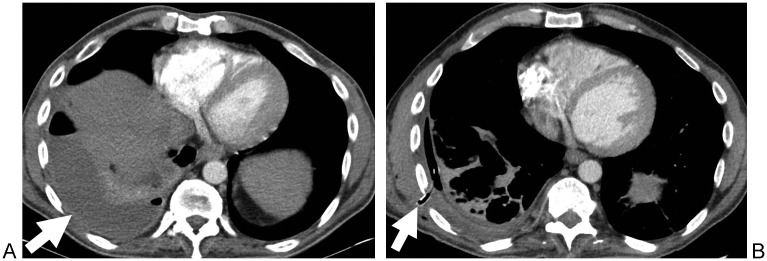
A 45-year-old man with fevers. (A) Axial contrast-enhanced computed tomography (CT) scan of the chest demonstrates a right empyema (arrow). (B) Axial CT scan of the chest after chest tube placement (arrow) and administration of six doses of tissue plasminogen activator. The right empyema shows near complete resolution.
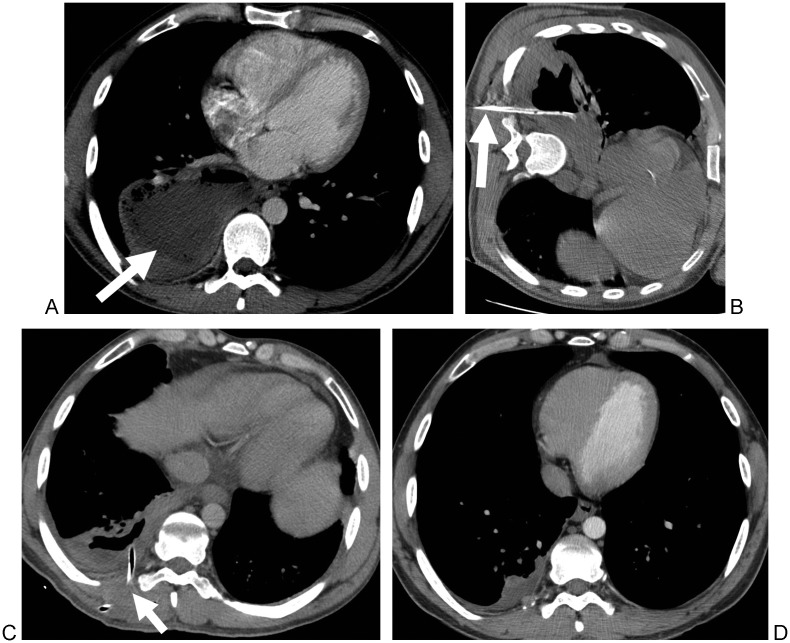
A 26-year-old man with a history of intravenous drug abuse who failed conservative management. (A) Axial contrast-enhanced computed tomography (CT) scan of the chest demonstrates a right lower lobe pulmonary abscess (arrow). (B) Axial CT scan of the chest with the patient in a lateral decubitus position that demonstrates the catheter (arrow) in the abscess. (C). Axial CT scan of the chest obtained 4 days later demonstrates the catheter in the abscess (arrow) and a significant decrease in the size of the abscess. (D) Axial CT scan of the chest obtained 2 months after drainage shows residual right pleural thickening but no residual abscess.
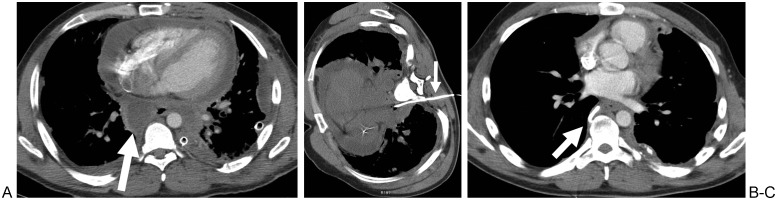
A 39-year-old man status post repair of an emetogenic esophageal perforation. (A) Axial contrast-enhanced computed tomography (CT) scan of the chest demonstrates a posterior mediastinal abscess (arrow). (B) Axial CT scan of the chest with the patient in a lateral decubitus position demonstrates the catheter in the abscess (arrow) while avoiding the lung and pleura. (C) Axial CT scan of the chest obtained 2 weeks after drainage demonstrates near complete resolution of the abscess (arrow).
References
-
- Weldon E Williams J Pleural disease in the emergency department Emerg Med Clin North Am 2012302475–499., ix–x - PubMed
-
- Light R W, Macgregor M I, Luchsinger P C, Ball W C Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med. 1972;77(4):507–513. - PubMed
-
- Heffner J E. Discriminating between transudates and exudates. Clin Chest Med. 2006;27(2):241–252. - PubMed
-
- Light R W. Parapneumonic effusions and empyema. Clin Chest Med. 1985;6(1):55–62. - PubMed
-
- Daniels C E, Ryu J H. Improving the safety of thoracentesis. Curr Opin Pulm Med. 2011;17(4):232–236. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
