

Review
doi: 10.1055/s-0032-1330064.
Image-guided percutaneous splenic biopsy and drainage
Affiliations
- PMID: 24293803
- PMCID: PMC3577624
- DOI: 10.1055/s-0032-1330064
Item in Clipboard
Review
Image-guided percutaneous splenic biopsy and drainage
Semin Intervent Radiol.
2012 Dec.
Abstract
Percutaneous splenic biopsy and drainage are relatively safe and accurate procedures. The risk of major complication (1.3%) following percutaneous splenic biopsy does not exceed that of other solid intra-abdominal organ biopsies, and it has less morbidity and mortality than splenectomy. Both computed tomography and ultrasound can be used to provide image guidance for biopsy and drainage. The safety profile of fine-needle aspiration cytology is better than core needle biopsy, but core biopsy has superior diagnostic accuracy.
Keywords: biopsy; computed tomography; drainage; interventional radiology; spleen; ultrasound.
Figures

Splenic biopsy in a 75-year-old man with splenomegaly due to marginal zone lymphoma. (A) Ultrasound-guided fine-needle aspiration and core biopsy (arrow) demonstrated no malignancy. (B) Computed tomography performed 3 hours subsequent to biopsy due to pain showed no hematoma around the spleen (arrow). Subsequent elective splenectomy showed marginal zone lymphoma at pathology.
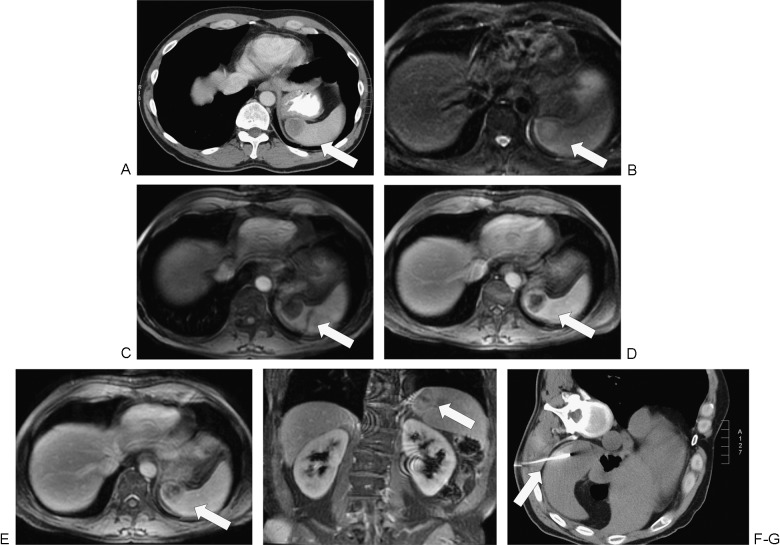
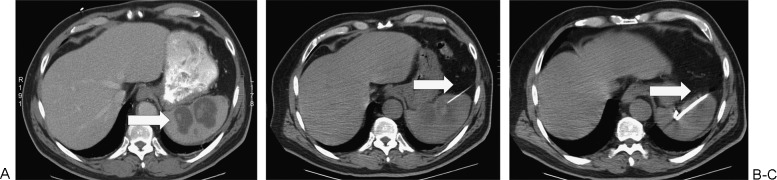
Splenic biopsy in a 45-year-old man with metastatic disease to the spleen from non–small cell lung cancer. (A) Staging computed tomography (CT) demonstrates a hypoattenuating lesion in the liver spleen (arrow) but no suspicion for other organ metastases. (B) T2 fat-saturated magnetic resonance imaging (MRI) demonstrates a hyperintense lesion in the spleen (arrow) that distorts the splenic contour. (C) The lesion is hypointense (arrow) on T1-weighted MRI. (D) Delayed (portal venous phase) post contrast imaging shows heterogenous enhancement of the mass (arrow). (E, F) More delayed imaging (180 seconds post contrast administration) in the axial and coronal planes demonstrates washout of the periphery of the lesion (arrow). (G) The lesion was suspicious for metastasis by imaging, and the spleen was the only site of metastatic disease. Splenic biopsy was performed under CT guidance (arrow), which confirmed the diagnosis of metastatic lung carcinoma.
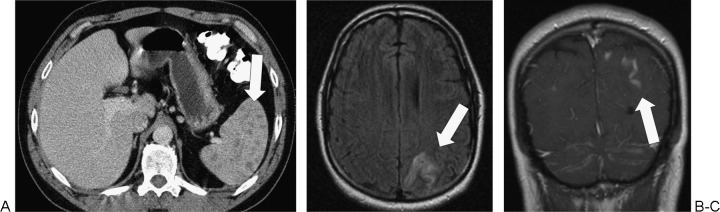
Cryptococcus of spleen and meninges in a 44-year-old man with CD4 lymphopenia (not related to human immunodeficiency virus). (A) Axial computed tomography (CT) of the abdomen demonstrates multiple tiny splenic hypodensities (arrow). (B) Axial fluid attenuated inversion recovery magnetic resonance imaging (MRI) of the brain demonstrates hyperintensity in the left posterior parietal cortex (arrow). (C) Coronal post intravenous contrast MRI of the brain demonstrates leptomeningeal enhancement compatible with cryptococcus infection(arrow).

Splenic biopsy in a 35-year-old woman with multiple splenic lesions due to sarcoidosis. (A) Axial computed tomography demonstrates multiple small hypoenhancing splenic lesions (arrow). (B) The lesions are fluorodeoxyglucose (FDG) avid on positron emission tomography scan (arrow). There were no other areas of abnormal increased FDG uptake. (C) Ultrasound-guided splenic biopsy was performed (arrow), and the diagnosis of sarcoidosis was confirmed.

Biopsy of spleen in a man with a history of alcohol abuse. (A) He presented with a psoas abscess, pyrexia, and multiple splenic lesions (arrow). (B) Computed tomography guided fine-needle aspiration cytology and core biopsy (arrow) did not show malignancy or infection. (C) Gelfoam (arrow) was injected along the needle tract at the end of the procedure. The patient succumbed to multiorgan failure; multiple hamartomas were diagnosed at autopsy.

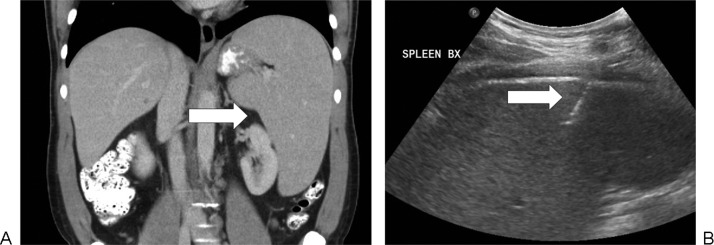
Splenic biopsy in a 53-year-old man with anemia and splenomegaly, hepatitis C, metastatic testicular seminoma, and renal insufficiency with prior failed renal transplant. (A) There was uniformly mildly increased fluorodeoxyglucose uptake in the spleen (arrow). (B) Fine-needle aspiration cytology and core biopsy (arrow) demonstrated extramedullary hematopoiesis. (C) The patient had perisplenic hematoma (arrow) after biopsy that was successfully treated medically. The patient had a splenectomy 2 months later due to persistent concerns for lymphoma, but the diagnosis of extramedullary hematopoiesis was confirmed following surgical resection.
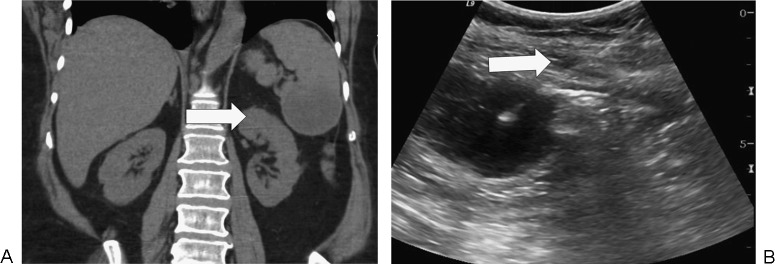
Splenic biopsy in a 41-year-old man with splenomegaly and pancytopenia. (A) Axial computed tomography demonstrates a uniformly enlarged spleen (arrow) without focal mass. (B) Ultrasound-guided fine-needle aspiration cytology and needle core biopsy (arrow) was inconclusive. Chronic lymphocytic lymphoma was diagnosed following splenectomy.

Splenic biopsy in a 66-year-old woman with splenomegaly due to lymphoma. (A) Axial computed tomography (CT) demonstrates splenomegaly and a hypoenhancing infiltrative process (arrow). (B) CT-guided fine-needle aspiration cytology and core biopsy of the spleen (arrow) showed fibrosis and necrosis. Subsequent splenectomy demonstrated lymphoma.

Positron emission tomography (PET) scan and computed tomography (CT) of the abdomen in a 73-year-old woman with chronic lymphocytic lymphoma. (A) There is avid fluorodeoxyglucose uptake in the spleen on PET (arrow). (B) There are multiple tiny nodules in the spleen (arrow) on contrast-enhanced CT.

Splenic drainage in a 71-year-old woman with splenic abscess following resection of a left lower lobe metastatic deposit from pancreatic cancer complicated by diaphragmatic injury. (A) Axial computed tomography (CT) demonstrates a collection in the spleen (arrow) and around the spleen (arrowhead). (B) Drainage catheter was inserted by tandem trochar technique under CT guidance.
Splenic abscess drainage in a 66-year-old woman with small bowel obstruction due to a cecal mass. (A) There is a collection (arrow) in the lower spleen on coronal noncontrast computed tomography. (B) Drainage catheter (arrow) was inserted under ultrasound guidance.
Splenic abscess drainage in a 67-year-old woman. (A) There is a bilobed collection (arrow) in the spleen on axial computed tomography (CT). (B) A 20-gauge Chiba needle (arrow) placed first under CT guidance. (C) Catheter (arrow) placed by tandem trochar technique under CT guidance.

Splenic abscess drainage in a 46-year-old man who presented with abdominal pain due to splenic abscess, later attributed to infective endocarditis. (A) Drainage catheter (arrow) was inserted on the computed tomography (CT) table under ultrasound guidance. (B) CT confirmed catheter position (arrow) prior to aspiration.
References
-
- Bhatia K, Sahdev A, Reznek R H. Lymphoma of the spleen. Semin Ultrasound CT MR. 2007;28(1):12–20. - PubMed
-
- Kamaya A, Weinstein S, Desser T S. Multiple lesions of the spleen: differential diagnosis of cystic and solid lesions. Semin Ultrasound CT MR. 2006;27(5):389–403. - PubMed
-
- McInnes M D, Kielar A Z, Macdonald D B. Percutaneous image-guided biopsy of the spleen: systematic review and meta-analysis of the complication rate and diagnostic accuracy. Radiology. 2011;260(3):699–708. - PubMed
-
- Tam A, Krishnamurthy S, Pillsbury E P. et al.Percutaneous image-guided splenic biopsy in the oncology patient: an audit of 156 consecutive cases. J Vasc Interv Radiol. 2008;19(1):80–87. - PubMed
-
- Lucey B C, Boland G W, Maher M M, Hahn P F, Gervais D A, Mueller P R. Percutaneous nonvascular splenic intervention: a 10-year review. AJR Am J Roentgenol. 2002;179(6):1591–1596. - PubMed
