

A Case Series of Uterine Rupture: Lessons to be Learned for Future Clinical Practice
- PMID: 24293845
- PMCID: PMC3575904
- DOI: 10.1007/s13224-012-0328-4
A Case Series of Uterine Rupture: Lessons to be Learned for Future Clinical Practice
Abstract
Objective: In this article, we try to discuss risk factors and diagnostic difficulties for uterine rupture.
Methods: Case series of 12 cases of uterine rupture observed in the Norfolk and Norwich University Hospital in the UK, with an average yearly birth rate of 6,000 deliveries, over a 6-year period.
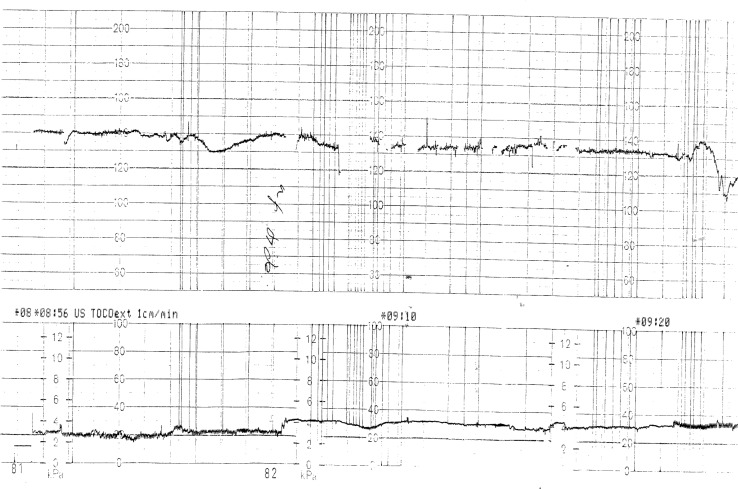
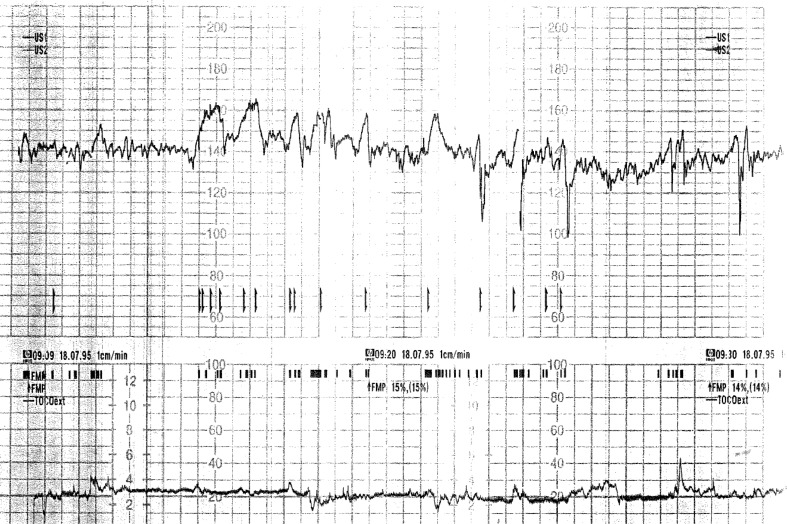
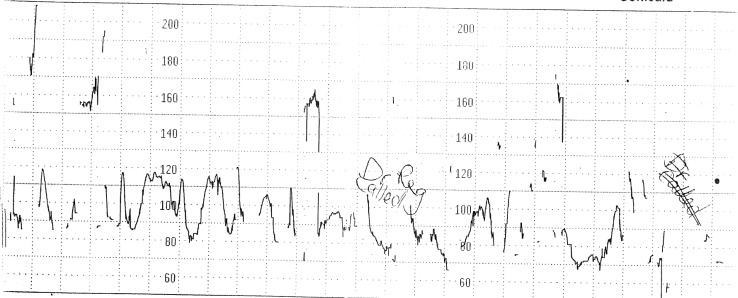
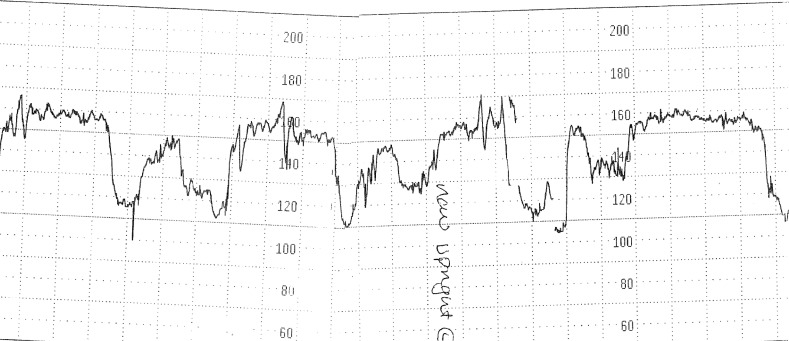
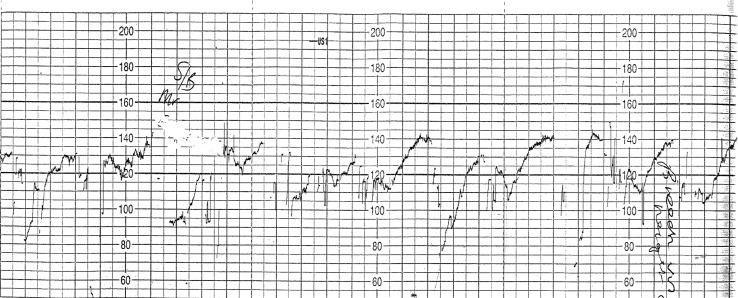
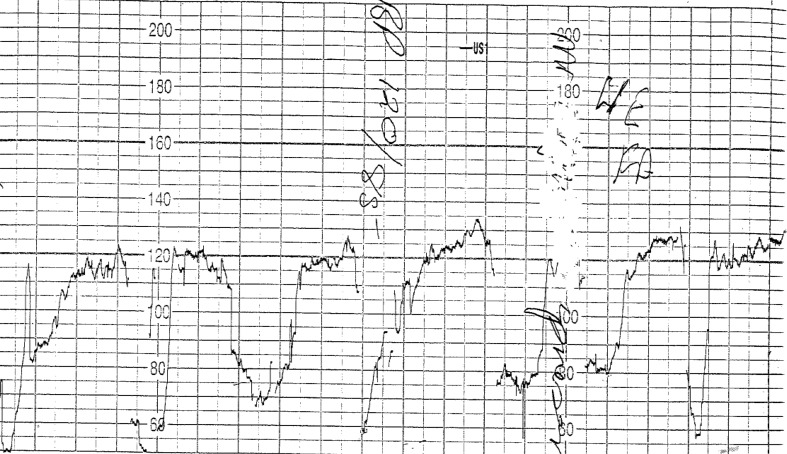
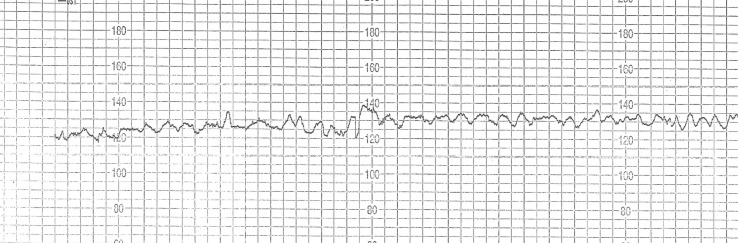
Results: In the present case series, there was no maternal mortality, and uterine rupture was a rare occurrence (12 in 36,000 births). Uterine rupture is associated with clinically significant uterine bleeding, fetal distress, expulsion or protrusion of the fetus, placenta or both into the abdominal cavity, and the need for prompt cesarean delivery and uterine repair or hysterectomy. The risk factors for rupture include previous cesarean sections, multiparity, malpresentation and obstructed labor, uterine anomalies, and use of prostaglandins for induction of labor. Previous cesarean section is, however, the most commonly associated risk factor. The most consistent early indicator of uterine rupture is the onset of a prolonged, persistent, and profound fetal bradycardia.
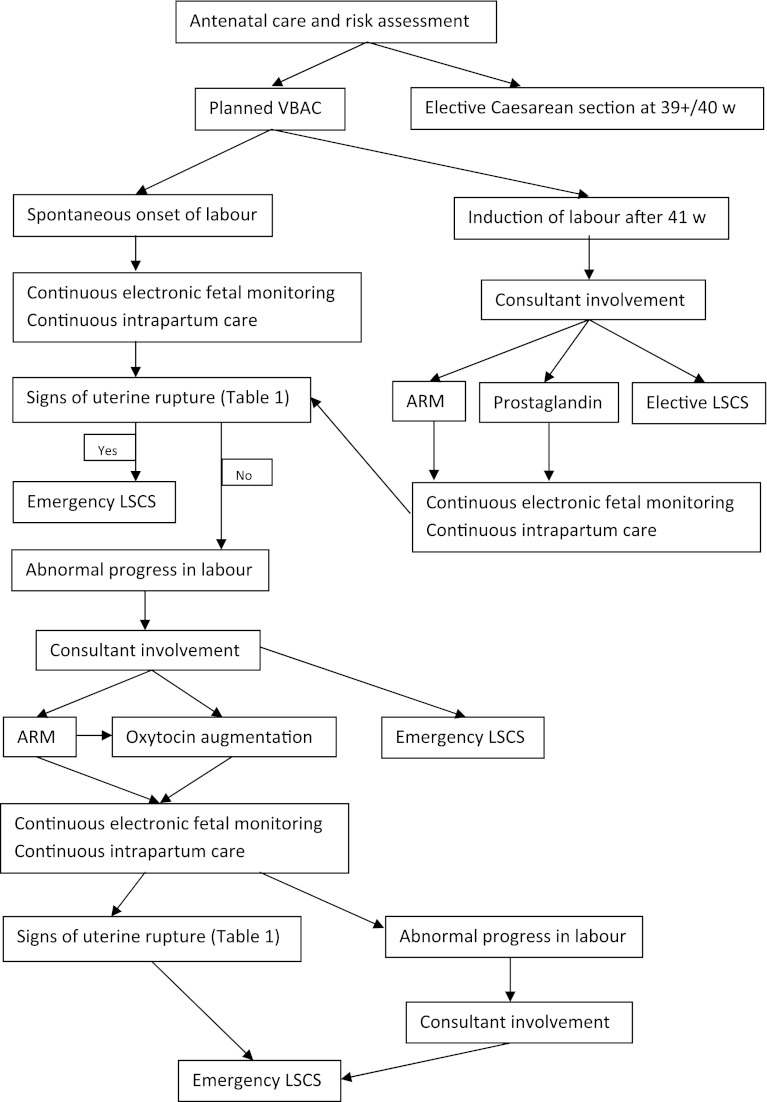
Conclusion: In this case series, we suggest that the signs and symptoms of uterine rupture are typically nonspecific, which makes diagnosis difficult. Delay in definitive therapy causes significant fetal morbidity. The inconsistent signs and the short time in prompting definitive treatment of uterine rupture make it a challenging event. For the best outcome, vaginal birth after previous cesarean section needs to be looked after in an appropriately staffed and equipped unit for an immediate cesarean delivery and advanced neonatal support.
Keywords: Previous cesarean section; Prolonged bradycardia; Risk factor; Uterine rupture.
Figures
Similar articles
-
Diagnosis and Management of Uterine Rupture in the Third Trimester of Pregnancy: A Case Series and Literature Review.Cureus. 2023 Jun 2;15(6):e39861. doi: 10.7759/cureus.39861. eCollection 2023 Jun. Cureus. 2023. PMID: 37404397 Free PMC article.
-
Delivery for women with a previous cesarean: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2013 Sep;170(1):25-32. doi: 10.1016/j.ejogrb.2013.05.015. Epub 2013 Jun 28. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 23810846 Review.
-
Maternal and neonatal outcomes after uterine rupture in labor.Am J Obstet Gynecol. 2001 Jun;184(7):1576-81. doi: 10.1067/mob.2001.114855. Am J Obstet Gynecol. 2001. PMID: 11408884
-
[Clinical study on 67 cases with uterine rupture].Zhonghua Fu Chan Ke Za Zhi. 2014 May;49(5):331-5. Zhonghua Fu Chan Ke Za Zhi. 2014. PMID: 25030728 Chinese.
-
SOGC clinical practice guidelines. Guidelines for vaginal birth after previous caesarean birth. Number 155 (Replaces guideline Number 147), February 2005.Int J Gynaecol Obstet. 2005 Jun;89(3):319-31. doi: 10.1016/j.ijgo.2005.03.015. Int J Gynaecol Obstet. 2005. PMID: 16001462 Review.
Cited by
-
Uterine rupture in the first trimester: a case report and review of the literature.J Med Case Rep. 2024 Jan 6;18(1):5. doi: 10.1186/s13256-023-04318-w. J Med Case Rep. 2024. PMID: 38183151 Free PMC article. Review.
-
First Trimester Uterine Rupture, a Rare but Life-Threatening Event: A Case Report.Iran J Med Sci. 2019 Sep;44(5):422-426. doi: 10.30476/IJMS.2019.44948. Iran J Med Sci. 2019. PMID: 31582867 Free PMC article.
-
Prevalence and associated factors of birth asphyxia among live births at Debre Tabor General Hospital, North Central Ethiopia.BMC Pregnancy Childbirth. 2020 Oct 28;20(1):653. doi: 10.1186/s12884-020-03348-2. BMC Pregnancy Childbirth. 2020. PMID: 33115413 Free PMC article.
-
Risk Factors of Birth Asphyxia among Newborns at Debre Markos Comprehensive Specialized Referral Hospital, Northwest Ethiopia: Unmatched Case-Control Study.Ethiop J Health Sci. 2022 May;32(3):513-522. doi: 10.4314/ejhs.v32i3.6. Ethiop J Health Sci. 2022. PMID: 35813672 Free PMC article.
-
Understanding of Key Obstetric Quality Terminology by Asian and Pacific Islander Subgroups: Implications for Patient Engagement and Health Equity.Matern Child Health J. 2018 Nov;22(11):1543-1549. doi: 10.1007/s10995-018-2597-8. Matern Child Health J. 2018. PMID: 30006728
References
Publication types
LinkOut - more resources
Full Text Sources