

The usefulness of F-18 FDG PET/CT-mammography for preoperative staging of breast cancer: comparison with conventional PET/CT and MR-mammography
- PMID: 24294185
- PMCID: PMC3814285
- DOI: 10.2478/raon-2013-0031
The usefulness of F-18 FDG PET/CT-mammography for preoperative staging of breast cancer: comparison with conventional PET/CT and MR-mammography
Abstract
Background: The objective of the study was to compare the diagnostic efficacy of an integrated Fluorine-18 fluorodeoxyglucose (F-18 FDG) PET/CT-mammography (mammo-PET/CT) with conventional torso PET/CT (supine-PET/CT) and MR-mammography for initial assessment of breast cancer patients.
Patients and methods: Forty women (52.0 ± 12.0 years) with breast cancer who underwent supine-PET/CT, mammo-PET/CT, and MR-mammography from April 2009 to August 2009 were enrolled in the study. We compared the size of the tumour, tumour to chest wall distance, tumour to skin distance, volume of axillary fossa, and number of meta-static axillary lymph nodes between supine-PET/CT and mammo-PET/CT. Next, we assessed the difference of focality of primary breast tumour and tumour size in mammo-PET/CT and MR-mammography. Histopathologic findings served as the standard of reference.
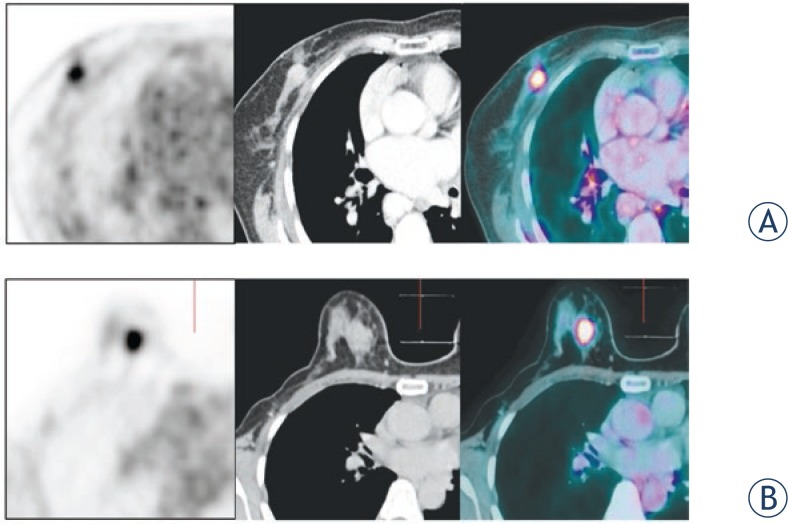
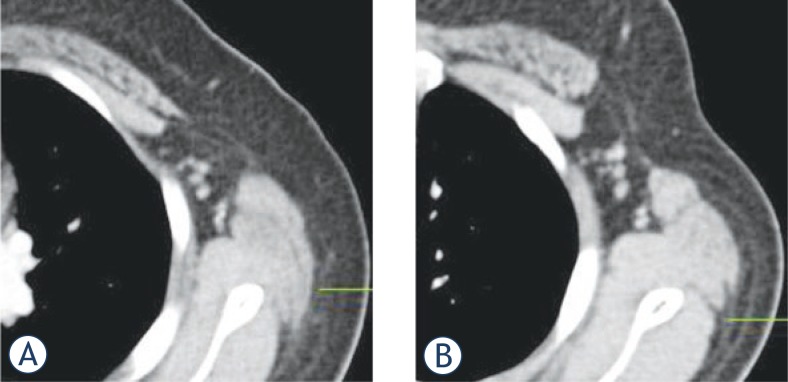
Results: In the comparison between supine-PET/CT and mammo-PET/CT, significant differences were found in the tumour size (supine-PET/CT: 1.3 ± 0.6 cm, mammo-PET/CT: 1.5 ± 0.6 cm, p < 0.001), tumour to thoracic wall distance (1.8 ± 0.9 cm, 2.2 ± 2.1 cm, p < 0.001), and tumour to skin distance (1.5 ± 0.8 cm, 2.1 ± 1.4 cm, p < 0.001). The volume of axillary fossa was significantly wider in mammo-PET/CT than supine-PET/CT (21.7 ± 8.7 cm(3) vs. 23.4 ± 10.4 cm(3), p = 0.03). Mammo-PET/CT provided more correct definition of the T-stage of the primary tumour than did supine-PET/CT (72.5% vs. 67.5%). No significant difference was found in the number of metastatic axillary lymph nodes. Compared with MR-mammography, mammo-PET/CT provided more correct classification of the focality of lesion than did MR-mammography (95% vs. 90%). In the T-stage, 72.5% of cases with mammo-PET/CT and 70% of cases with MR-mammography showed correspondence with pathologic results.
Conclusions: Mammo-PET/CT provided more correct definition of the T-stage and evaluation of axillary fossa may also be delineated more clearly than with supine-PET/CT. The initial assessment of mammo-PET/CT would be more useful than MR-mammography because the mammo-PET/CT indicates similar accuracy with MR-mammography for decision of T-stage of primary breast tumour and more correct than MR-mammography for defining focality of lesion.
Keywords: MRI; breast cancer; fluorodeoxyglucose; mammography; positron emission tomography.
Figures

Similar articles
-
Potential Clinical Applications of 18F-Fluorodeoxyglucose Positron Emission Tomography/Magnetic Resonance Mammography in Breast Cancer.Nucl Med Mol Imaging. 2017 Sep;51(3):217-226. doi: 10.1007/s13139-016-0446-5. Epub 2016 Aug 30. Nucl Med Mol Imaging. 2017. PMID: 28878847 Free PMC article. Review.
-
Breast cancer staging in a single session: whole-body PET/CT mammography.J Nucl Med. 2008 Aug;49(8):1215-22. doi: 10.2967/jnumed.108.052050. Epub 2008 Jul 16. J Nucl Med. 2008. PMID: 18632831
-
Whole-body FDG PET/CT is more accurate than conventional imaging for staging primary breast cancer patients.Eur J Nucl Med Mol Imaging. 2012 May;39(5):852-63. doi: 10.1007/s00259-012-2077-0. Epub 2012 Mar 6. Eur J Nucl Med Mol Imaging. 2012. PMID: 22392069
-
Whole-body PET/CT-mammography for staging breast cancer: initial results.Br J Radiol. 2008 Sep;81(969):743-8. doi: 10.1259/bjr/69647413. Epub 2008 May 28. Br J Radiol. 2008. PMID: 18508873
-
Locoregional tumour evaluation of squamous cell carcinoma in the head and neck area: a comparison between MRI, PET/CT and integrated PET/MRI.Eur J Nucl Med Mol Imaging. 2016 Jan;43(1):92-102. doi: 10.1007/s00259-015-3145-z. Epub 2015 Aug 6. Eur J Nucl Med Mol Imaging. 2016. PMID: 26243264
Cited by
-
Thyroid lesions incidentally detected by (18)F-FDG PET-CT - a two centre retrospective study.Radiol Oncol. 2015 Mar 25;49(2):121-7. doi: 10.2478/raon-2014-0039. eCollection 2015 Jun. Radiol Oncol. 2015. PMID: 26029022 Free PMC article.
-
Potential Clinical Applications of 18F-Fluorodeoxyglucose Positron Emission Tomography/Magnetic Resonance Mammography in Breast Cancer.Nucl Med Mol Imaging. 2017 Sep;51(3):217-226. doi: 10.1007/s13139-016-0446-5. Epub 2016 Aug 30. Nucl Med Mol Imaging. 2017. PMID: 28878847 Free PMC article. Review.
-
Investigation of Added Value of Imaging Performed in a Prone Position to Standard 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography Imaging for Staging in Patients with Breast Cancer.Mol Imaging Radionucl Ther. 2022 Feb 2;31(1):23-32. doi: 10.4274/mirt.galenos.2021.48343. Mol Imaging Radionucl Ther. 2022. PMID: 35114748 Free PMC article.
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–30. - PubMed
-
- Kopans DB. The positive predictive value of mammography. Am J Roentgenol. 1992;158:521–6. - PubMed
-
- Bird RE, Wallace TW, Yankaskas BC. Analysis of cancer missed at screening mammography. Radiology. 1992;184:613–7. - PubMed
-
- Adriaenssens N, Belsack D, Buyl R, Ruggiero L, Breucq C, De Mey J, Lievens P, Lamote J. Ultrasound elastography as an objective diagnostic measurement tool for lymphoedema of the treated breast in breast cancer patients following breast conserving surgery and radiotherapy. Radiol Oncol. 2012;46:284–95. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous