

Penicillin susceptibility and macrolide-lincosamide-streptogramin B resistance in group B Streptococcus isolates from a Canadian hospital
- PMID: 24294274
- PMCID: PMC3597397
- DOI: 10.1155/2012/540127
Penicillin susceptibility and macrolide-lincosamide-streptogramin B resistance in group B Streptococcus isolates from a Canadian hospital
Abstract
Background: Intrapartum antibiotic prophylaxis (IAP) is recommended for pregnant women who test positive for group B Streptococcus (GBS) in their genitourinary tract to prevent GBS-induced neonatal sepsis. Penicillin G is used as the primary antibiotic, and clindamycin or erythromycin as the secondary, if allergies exist. Decreased susceptibility to penicillin G has occasionally been reported; however, clindamycin and erythromycin resistance is on the rise and is causing concern over the use of clindamycin and erythromycin IAP.
Methods: Antibiotic resistance was characterized phenotypically using a D-Test for erythromycin and clindamycin, while an E-Test (E-strip) was used for penicillin G. GBS was isolated from vaginal-rectal swabs and serologically confirmed using Prolex (Pro-Lab Diagnostics, Canada) streptococcal grouping reagents. Susceptibility testing of isolates was performed according to the Clinical Laboratory Standards Institute guidelines.
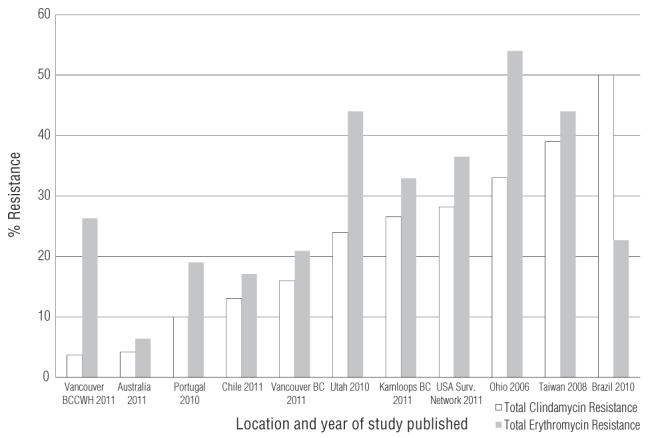
Results: All 158 isolates were penicillin G sensitive. Inducible macrolide-lincosamide-streptogramin B (MLSB) resistance was observed in 13.9% of isolates. Constitutive MLSB resistance was observed in 12.7% of isolates. M phenotype resistance was observed in 6.3% of isolates. In total, erythromycin resistance was present in 32.9% of the GBS isolates, while clindamycin resistance was present in 26.6%.
Discussion: The sampled GBS population showed no sign of reduced penicillin susceptibility, with all being well under susceptible minimum inhibitory concentration values. These data are congruent with the large body of evidence showing that penicillin G remains the most reliable clinical antibiotic for IAP. Clindamycin and erythromycin resistance was higher than expected, contributing to a growing body of evidence that suggests the re-evaluation of clindamycin and erythromycin IAP is warranted.
Historique: La prophylaxie antibiotique intrapartum (PAI) est recommandée chez les femmes enceintes positives au Streptococcus du groupe B (SGB) dans l’appareil génito-urinaire, afin de prévenir la septicémie néonatale induite par le SGB. La pénicilline G est utilisée comme antibiotique primaire et, en cas d’allergies, la clindamycine ou l’érythromycine comme antibiotique secondaire. On déclare parfois une diminution de la susceptibilité à la pénicilline G, mais la résistance à la clindamycine et à l’érythromycine est à la hausse et suscite des inquiétudes quant à leur utilisation en PAI.
Méthodologie: Les chercheurs ont caractérisé les phénotypes de résistance aux antibiotiques au moyen d’un test de diffusion pour l’érythromycine et la clindamycine et d’un test E (bandelette E) pour la pénicilline G. Ils ont isolé le SGB dans les écouvillons vagino-rectaux et en ont fait la confirmation sérologique au moyen des réactifs de groupement streptococcique Prolex (Pro-Lab Diagnostics, Canada). Les tests de susceptibilité des isolats ont été exécutés conformément aux lignes directrices du Clinical Laboratory Standards Institute.
Résultats: Les 158 isolats étaient sensibles à la pénicilline G. Les chercheurs ont observé une résistance au macrolide, à la lincosamide et à la streptogramine de type B (MLSB) dans 13,9 % des isolats. Ils ont observé une résistance à MLSB dans 12,7 % des isolats et la résistance au phénotype M dans 6,3 % des isolats. Au total, ils ont constaté une résistance à l’érythromycine dans 32,9 % des isolats de SGB, et une résistance à la clindamycine dans 26,6 % des cas.
Exposé: L’échantillon de population atteint du SGB n’a révélé aucun signe de diminution de la susceptibilité à la pénicilline, car tous les sujets se situaient bien en deçà des valeurs CMI susceptibles. Ces données coïncident avec le vaste ensemble de données probantes démontrant que la pénicilline G demeure l’antibiotique clinique le plus fiable pour la PIA. La résistance à la clindamycine et à l’érythromycine était plus élevée que prévu, ce qui contribue à l’ensemble croissant de données probantes indiquant qu’il faut réévaluer la PIA à la clindamycine et à l’érythromycine.
Keywords: Clindamycin; Erythromycin; Group B Streptococcus; Macrolide-lincosamide-streptogramin B resistance; Penicillin resistance; Regional hospital.
Figures
Similar articles
-
Group B streptococcus colonization of Romanian women: phenotypic traits of isolates from vaginal swabs.Roum Arch Microbiol Immunol. 2009 Oct-Dec;68(4):235-9. Roum Arch Microbiol Immunol. 2009. PMID: 20583478
-
Point prevalence study of antibiotic susceptibility of genital group B streptococcus isolated from near-term pregnant women in Calgary, Alberta.Can J Infect Dis Med Microbiol. 2012 Fall;23(3):121-4. doi: 10.1155/2012/876103. Can J Infect Dis Med Microbiol. 2012. PMID: 23997778 Free PMC article.
-
Survey of strain distribution and antibiotic resistance pattern of group B streptococci (Streptococcus agalactiae) isolated from clinical specimens.GMS Hyg Infect Control. 2016 Sep 12;11:Doc18. doi: 10.3205/dgkh000278. eCollection 2016. GMS Hyg Infect Control. 2016. PMID: 27648402 Free PMC article.
-
Prevention of group B streptococcal disease in the newborn.Am Fam Physician. 2005 Mar 1;71(5):903-10. Am Fam Physician. 2005. PMID: 15768620 Review.
-
Acquired resistance to macrolide-lincosamide-streptogramin antibiotics in lactic Acid bacteria of food origin.Indian J Microbiol. 2012 Dec;52(4):530-7. doi: 10.1007/s12088-012-0296-5. Epub 2012 Aug 9. Indian J Microbiol. 2012. PMID: 24293706 Free PMC article. Review.
Cited by
-
Invasive group B streptococcal infection in infants in Shenzhen, China.Int J Clin Exp Med. 2015 Feb 15;8(2):2939-43. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 25932259 Free PMC article.
-
Cloning, expression, purification, crystallization and preliminary X-ray diffraction analysis of glyceraldehyde-3-phosphate dehydrogenase from Streptococcus agalactiae NEM316.Acta Crystallogr F Struct Biol Commun. 2014 Jul;70(Pt 7):938-41. doi: 10.1107/S2053230X14011418. Epub 2014 Jun 18. Acta Crystallogr F Struct Biol Commun. 2014. PMID: 25005093 Free PMC article.
-
Recent development and fighting strategies for lincosamide antibiotic resistance.Clin Microbiol Rev. 2024 Jun 13;37(2):e0016123. doi: 10.1128/cmr.00161-23. Epub 2024 Apr 18. Clin Microbiol Rev. 2024. PMID: 38634634 Free PMC article. Review.
-
Drugs for the Prevention and Treatment of Sepsis in the Newborn.Clin Perinatol. 2019 Jun;46(2):327-347. doi: 10.1016/j.clp.2019.02.012. Epub 2019 Mar 30. Clin Perinatol. 2019. PMID: 31010563 Free PMC article. Review.
References
-
- Schrag S, Zywicki S, Farley M, et al. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med. 2000;342:15–20. - PubMed
-
- Franciosi RA, Knostman JD, Zimmerman RA. Group B streptococcal neonatal and infant infections. J Pediatr. 1973;82:707–18. - PubMed
-
- Society of Obstetricians and Gynaecologists of Canada and Canadian Paediatric Society National consensus statement on the prevention of early onset group B streptococcal infections in the newborn. J Obstet Gynaecol Can. 1994;16:2271–8.
-
- Society of Obstetricians and Gynaecologists of Canada Infectious Diseases Committee The prevention of early onset neonatal group B streptococcal disease. J Obstet Gynaecol Can. 2004;26:826–32. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
