

Catastrophic antiphospholipid syndrome: how to diagnose a rare but highly fatal disease
- PMID: 24294304
- PMCID: PMC3836378
- DOI: 10.1177/1759720X13502919
Catastrophic antiphospholipid syndrome: how to diagnose a rare but highly fatal disease
Abstract
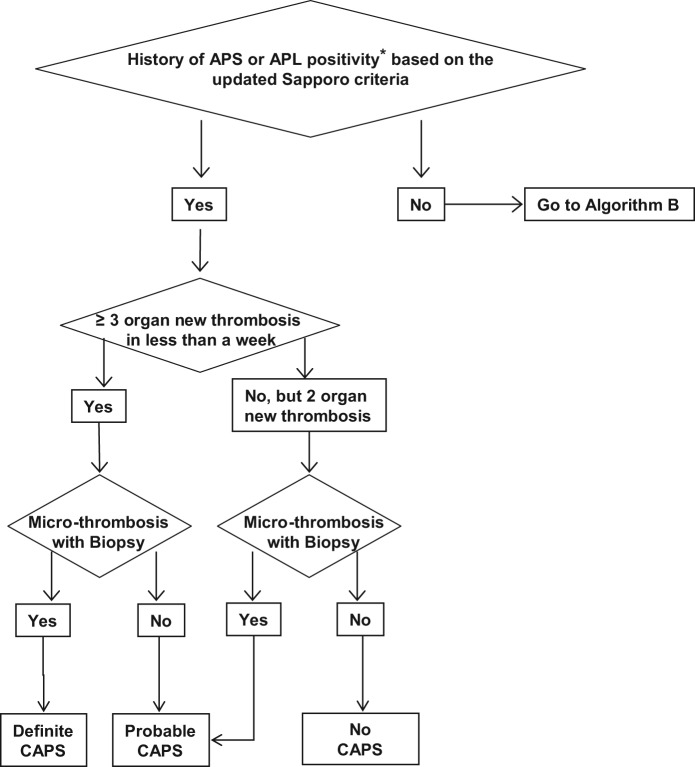
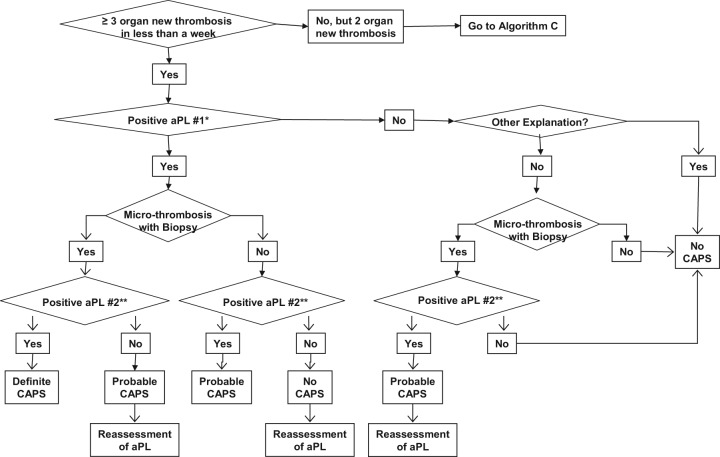
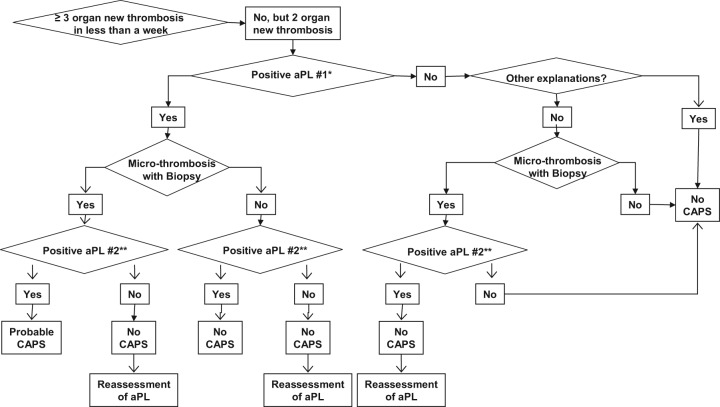
Antiphospholipid syndrome (APS) is a multisystem autoimmune condition characterized by vascular thromboses and/or pregnancy loss associated with persistently positive antiphospholipid antibodies (aPL). Catastrophic APS (CAPS) is the most severe form of APS with multiple organ involvement developing over a short period of time, usually associated with microthrombosis. 'Definite' and 'probable' CAPS have been defined based on the preliminary classification criteria; however, in a real-world setting, aPL-positive patients with multiple organ thromboses and/or thrombotic microangiopathies exist who do not fulfill these criteria. Previous APS diagnosis and/or persistent clinically significant aPL positivity is of great importance for the CAPS diagnosis; however, almost half of the patients who develop CAPS do not have a history of aPL positivity. The purpose of this paper is to summarize the diagnostic challenges and the recently updated diagnostic algorithms for CAPS providing a 'step-by-step' approach for clinicians (and researchers) in the assessment of patients with multiple organ thromboses.
Keywords: anti-β2-glycoprotein-1 antibody; anticardiolipin antibody; antiphospholipid syndrome; catastrophic antiphospholipid syndrome; lupus anticoagulant; thrombosis.
Conflict of interest statement
Figures
References
-
- Alpert D., Mandl L., Erkan D., Yin W., Peerschke E., Salmon J. (2008) Anti-heparin platelet factor 4 antibodies in systemic lupus erythematosus are associated with IgM antiphospholipid antibodies and the antiphospholipid syndrome. Ann Rheum Dis 67: 395–401 - PubMed
-
- Asherson R. (2006) New subsets of the antiphospholipid syndrome in 2006: “PRE-APS” (probable APS) and microangiopathic antiphospholipid syndromes (“MAPS”). Autoimmun Rev 6: 76–80 - PubMed
-
- Asherson R., Cervera R. (2008) Microvascular and microangiopathic antiphospholipid-associated syndromes (“MAPS”) semantic or antisemantic? Autoimmun Rev 7: 164–167 - PubMed
-
- Asherson R., Cervera R., de Groot P., Erkan D., Boffa M., Piette J., et al. (2003) Catastrophic antiphospholipid syndrome: international consensus statement on classification criteria and treatment guidelines. Lupus 12: 530–534 - PubMed
-
- Asherson R., Pierangeli S., Cervera R. (2007) Microangiopathic antiphospholipid associated syndromes revisited new concepts relating to antiphospholipid antibodies and syndromes. J Rheumatol 34: 1793–1795 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
