

In vivo diagnostic accuracy of high-resolution microendoscopy in differentiating neoplastic from non-neoplastic colorectal polyps: a prospective study
- PMID: 24296752
- PMCID: PMC3947255
- DOI: 10.1038/ajg.2013.387
In vivo diagnostic accuracy of high-resolution microendoscopy in differentiating neoplastic from non-neoplastic colorectal polyps: a prospective study
Abstract
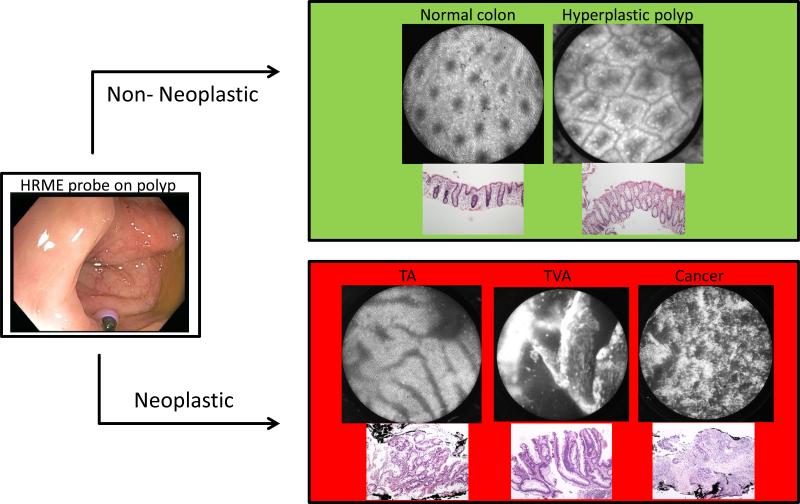
Objectives: High-resolution microendoscopy (HRME) is a low-cost, "optical biopsy" technology that allows for subcellular imaging. The purpose of this study was to determine the in vivo diagnostic accuracy of the HRME for the differentiation of neoplastic from non-neoplastic colorectal polyps and compare it to that of high-definition white-light endoscopy (WLE) with histopathology as the gold standard.
Methods: Three endoscopists prospectively detected a total of 171 polyps from 94 patients that were then imaged by HRME and classified in real-time as neoplastic (adenomatous, cancer) or non-neoplastic (normal, hyperplastic, inflammatory).
Results: HRME had a significantly higher accuracy (94%), specificity (95%), and positive predictive value (PPV, 87%) for the determination of neoplastic colorectal polyps compared with WLE (65%, 39%, and 55%, respectively). When looking at small colorectal polyps (less than 10 mm), HRME continued to significantly outperform WLE in terms of accuracy (95% vs. 64%), specificity (98% vs. 40%) and PPV (92% vs. 55%). These trends continued when evaluating diminutive polyps (less than 5 mm) as HRME's accuracy (95%), specificity (98%), and PPV (93%) were all significantly greater than their WLE counterparts (62%, 41%, and 53%, respectively).
Conclusions: In conclusion, this in vivo study demonstrates that HRME can be a very effective modality in the differentiation of neoplastic and non-neoplastic colorectal polyps. A combination of standard white-light colonoscopy for polyp detection and HRME for polyp classification has the potential to truly allow the endoscopist to selectively determine which lesions can be left in situ, which lesions can simply be discarded, and which lesions need formal histopathologic analysis.
Figures
References
-
- Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–81. - PubMed
-
- Vital signs: Colorectal cancer screening, incidence, and mortality--United States, 2002-2010. MMWR Morb Mortal Wkly Rep. 2011;60:884–9. - PubMed
-
- Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973-1997, with a special section on colorectal cancer. Cancer. 2000;88:2398–424. - PubMed
-
- Hawk ET, Levin B. Colorectal cancer prevention. J Clin Oncol. 2005;23:378–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
