

Etomidate use and postoperative outcomes among cardiac surgery patients
- PMID: 24296761
- PMCID: PMC3944222
- DOI: 10.1097/ALN.0000000000000087
Etomidate use and postoperative outcomes among cardiac surgery patients
Abstract
Background: Although a single dose of etomidate can cause relative adrenal insufficiency, the impact of etomidate exposure on postoperative outcomes is unknown. The objective of this study was to examine the association between a single induction dose of etomidate and clinically important postoperative outcomes after cardiac surgery.
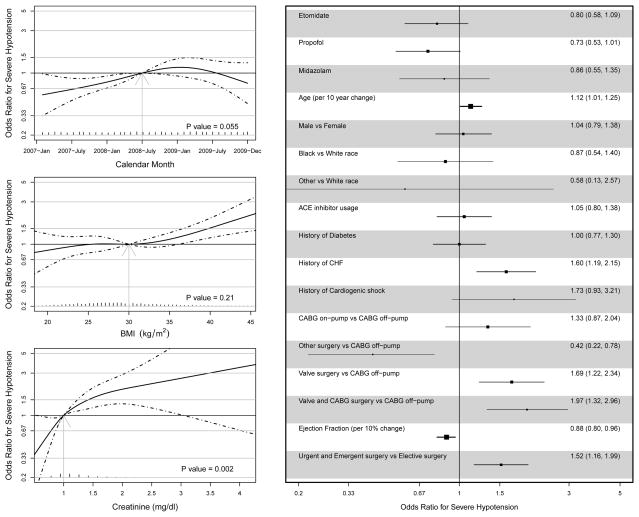
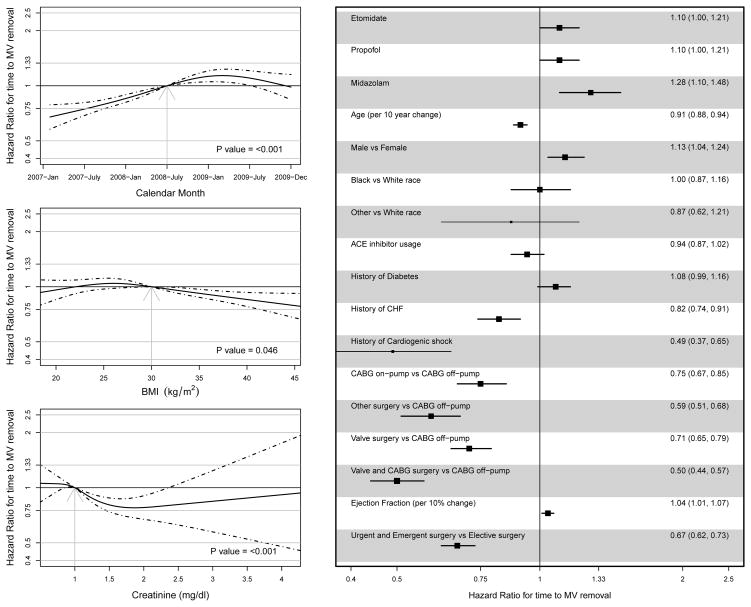
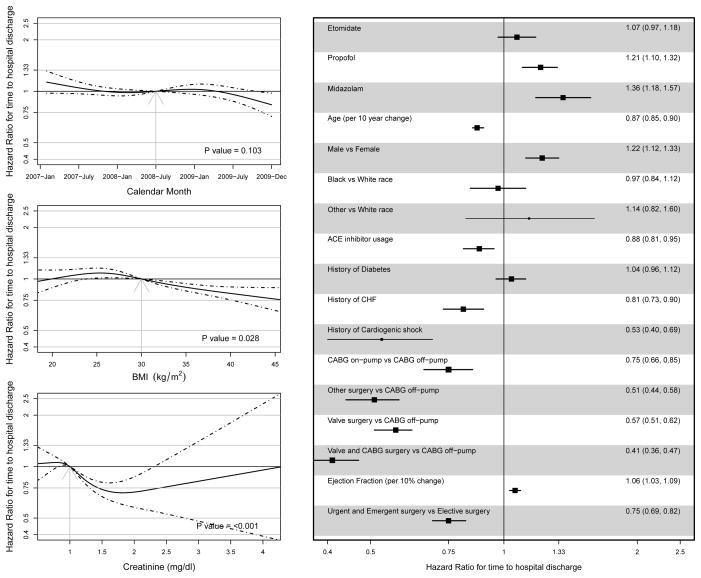
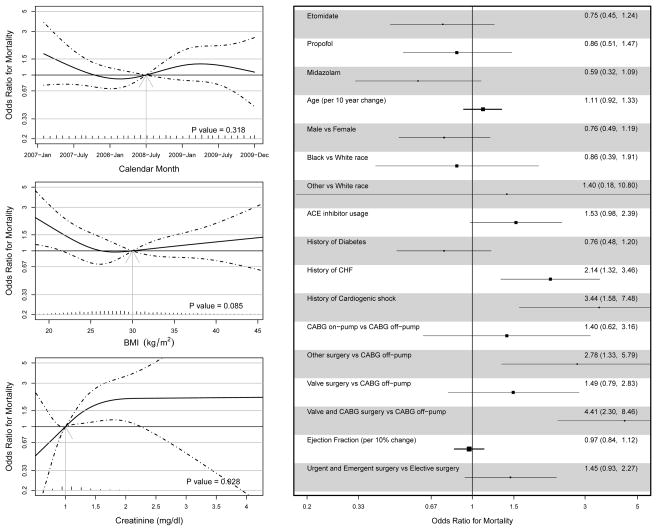
Methods: The authors retrospectively examined the association between etomidate exposure during induction of anesthesia and postoperative outcomes in patients undergoing cardiac surgery from January 2007 to December 2009 by using multivariate logistic regression analyses and Cox proportional hazards regression analyses. Postoperative outcomes of interest were severe hypotension, mechanical ventilation hours, hospital length of stay, and in-hospital mortality.
Results: Sixty-two percent of 3,127 patients received etomidate. Etomidate recipients had a higher incidence of preoperative congestive heart failure (23.0 vs. 18.3%; P = 0.002) and a lower incidence of preoperative cardiogenic shock (1.3 vs. 4.0%; P < 0.001). The adjusted odds ratio for severe hypotension and in-hospital mortality associated with receiving etomidate was 0.80 (95% CI, 0.58-1.09) and 0.75 (95% CI, 0.45-1.24), respectively, and the adjusted hazard ratio for time to mechanical ventilation removal and time to hospital discharge was 1.10 (95% CI, 1.00-1.21) and 1.07 (95% CI, 0.97-1.18), respectively. Propensity score analysis did not change the association between etomidate use and postoperative outcomes.
Conclusions: In this study, there was no evidence to suggest that etomidate exposure was associated with severe hypotension, longer mechanical ventilation hours, longer length of hospital stay, or in-hospital mortality. Etomidate should remain an option for induction of anesthesia in cardiac surgery patients.
Conflict of interest statement
The authors declare no competing interests
Figures
Comment in
-
Etomidate and treatment propensity.Anesthesiology. 2014 Nov;121(5):1128. doi: 10.1097/ALN.0000000000000417. Anesthesiology. 2014. PMID: 25335175 No abstract available.
-
In reply.Anesthesiology. 2014 Nov;121(5):1128-30. doi: 10.1097/ALN.0000000000000418. Anesthesiology. 2014. PMID: 25335176 No abstract available.
References
-
- Budde AO, Mets B. Pro: Etomidate is the ideal induction agent for a cardiac anesthetic. J Cardiothorac Vasc Anesth. 2013;27:180–3. - PubMed
-
- Cuthbertson BH, Sprung CL, Annane D, Chevret S, Garfield M, Goodman S, Laterre PF, Vincent JL, Freivogel K, Reinhart K, Singer M, Payen D, Weiss YG. The effects of etomidate on adrenal responsiveness and mortality in patients with septic shock. Intensive Care Med. 2009;35:1868–76. - PubMed
-
- Hohl CM, Kelly-Smith CH, Yeung TC, Sweet DD, Doyle-Waters MM, Schulzer M. The effect of a bolus dose of etomidate on cortisol levels, mortality, and health services utilization: A systematic review. Ann Emerg Med. 2010;56:105–13. e5. - PubMed
-
- Albert SG, Ariyan S, Rather A. The effect of etomidate on adrenal function in critical illness: A systematic review. Intensive Care Med. 2011;37:901–10. - PubMed
-
- Absalom A, Pledger D, Kong A. Adrenocortical function in critically ill patients 24 h after a single dose of etomidate. Anaesthesia. 1999;54:861–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
