

Atrial ectopy as a predictor of incident atrial fibrillation: a cohort study
- PMID: 24297188
- PMCID: PMC4115459
- DOI: 10.7326/0003-4819-159-11-201312030-00004
Atrial ectopy as a predictor of incident atrial fibrillation: a cohort study
Abstract
Background: Atrial fibrillation (AF) prediction models have unclear clinical utility given the absence of AF prevention therapies and the immutability of many risk factors. Premature atrial contractions (PACs) play a critical role in AF pathogenesis and may be modifiable.
Objective: To investigate whether PAC count improves model performance for AF risk.
Design: Prospective cohort study.
Setting: 4 U.S. communities.
Patients: A random subset of 1260 adults without prevalent AF enrolled in the Cardiovascular Health Study between 1989 and 1990.
Measurements: The PAC count was quantified by 24-hour electrocardiography. Participants were followed for the diagnosis of incident AF or death. The Framingham AF risk algorithm was used as the comparator prediction model.
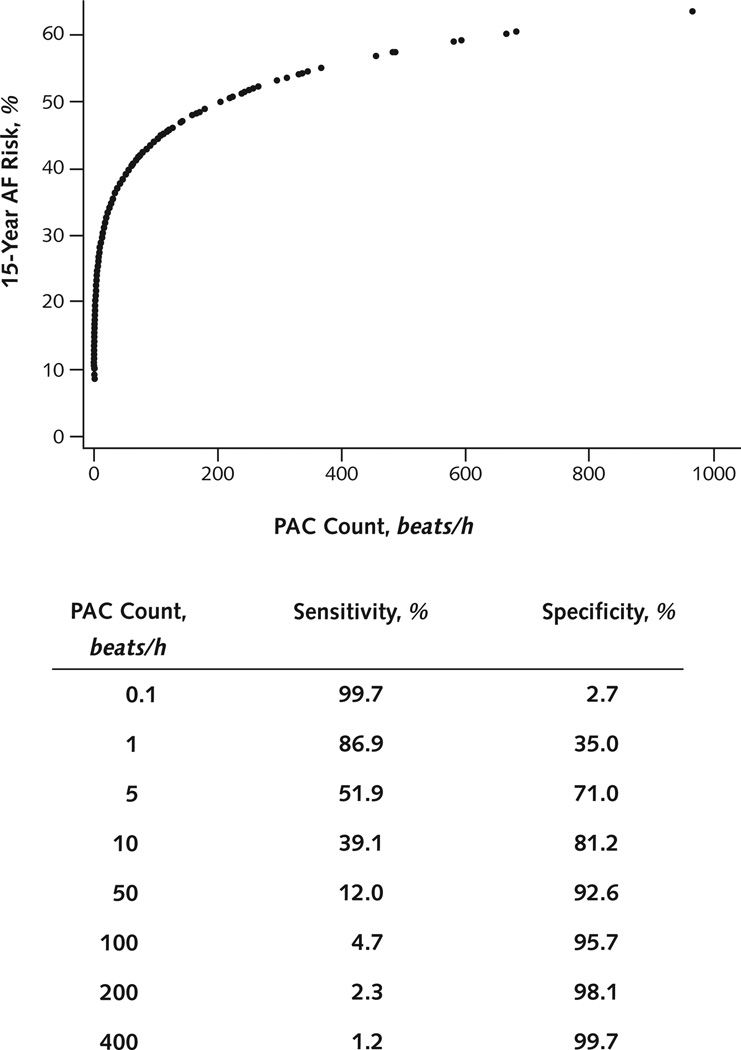
Results: In adjusted analyses, doubling the hourly PAC count was associated with a significant increase in AF risk (hazard ratio, 1.17 [95% CI, 1.13 to 1.22]; P < 0.001) and overall mortality (hazard ratio, 1.06 [CI, 1.03 to 1.09]; P < 0.001). Compared with the Framingham model, PAC count alone resulted in similar AF risk discrimination at 5 and 10 years of follow-up and superior risk discrimination at 15 years. The addition of PAC count to the Framingham model resulted in significant 10-year AF risk discrimination improvement (c-statistic, 0.65 vs. 0.72; P < 0.001), net reclassification improvement (23.2% [CI, 12.8% to 33.6%]; P < 0.001), and integrated discrimination improvement (5.6% [CI, 4.2% to 7.0%]; P < 0.001). The specificity for predicting AF at 15 years exceeded 90% for PAC counts more than 32 beats/h.
Limitation: This study does not establish a causal link between PACs and AF.
Conclusion: The addition of PAC count to a validated AF risk algorithm provides superior AF risk discrimination and significantly improves risk reclassification. Further study is needed to determine whether PAC modification can prospectively reduce AF risk.
Primary funding source: American Heart Association, Joseph Drown Foundation, and National Institutes of Health.
Conflict of interest statement
Figures

Comment in
-
Ectopy and expectations: can we predict atrial fibrillation, and should we try?Ann Intern Med. 2013 Dec 3;159(11):787-8. doi: 10.7326/0003-4819-159-11-201312030-00014. Ann Intern Med. 2013. PMID: 24297197 Free PMC article. No abstract available.
References
-
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol. 2009;104:1534–1539. [PMID: 19932788] - PubMed
-
- Lin HJ, Wolf PA, Kelly-Hayes M, Beiser AS, Kase CS, Benjamin EJ, et al. Stroke severity in atrial fibrillation. The Framingham Study. Stroke. 1996;27:1760–1764. [PMID: 8841325] - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–952. [PMID: 9737513] - PubMed
-
- Wolowacz SE, Samuel M, Brennan VK, Jasso-Mosqueda JG, Van Gelder IC. The cost of illness of atrial fibrillation: a systematic review of the recent literature. Europace. 2011;13:1375–1385. [PMID: 21757483] - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- R01HL116747/HL/NHLBI NIH HHS/United States
- N01 HC085082/HC/NHLBI NIH HHS/United States
- N01 HC085080/HC/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085086/HC/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- N01 HC085081/HC/NHLBI NIH HHS/United States
- N01HC85239/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HC/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- AG023629/AG/NIA NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- R01 HL116747/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical