

High prevalence of occult pulmonary venous hypertension revealed by fluid challenge in pulmonary hypertension
- PMID: 24297689
- PMCID: PMC3934572
- DOI: 10.1161/CIRCHEARTFAILURE.113.000468
High prevalence of occult pulmonary venous hypertension revealed by fluid challenge in pulmonary hypertension
Abstract
Background: Determining the cause for pulmonary hypertension is difficult in many patients. Pulmonary arterial hypertension (PAH) is differentiated from pulmonary venous hypertension (PVH) by a wedge pressure (PWP)>15 mm Hg in PVH. Patients undergoing right heart catheterization for evaluation of pulmonary hypertension may be dehydrated and have reduced intravascular volume, potentially leading to a falsely low measurement of PWP and an erroneous diagnosis of PAH. We hypothesized that a fluid challenge during right heart catheterization would identify occult pulmonary venous hypertension (OPVH).
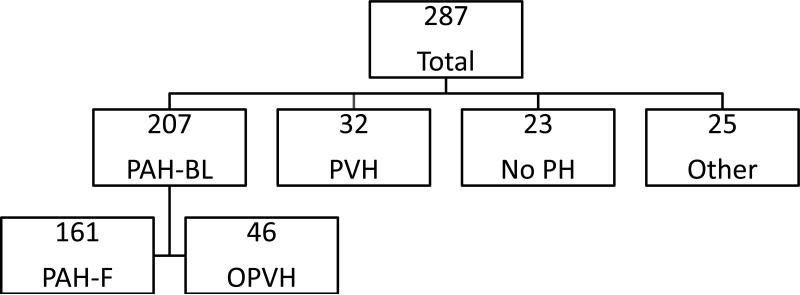
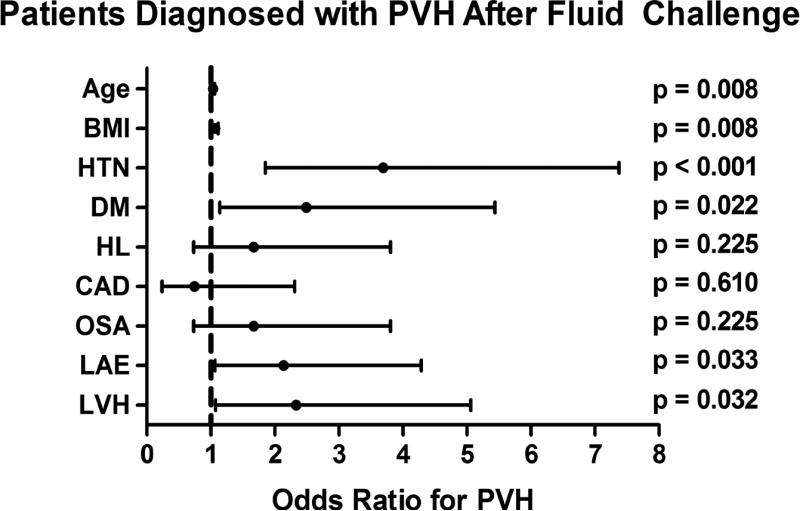
Methods and results: We reviewed the results of patients undergoing fluid challenge in our pulmonary hypertension database from 2004 to 2011. Baseline hemodynamics were obtained and repeated after infusion of 0.5 L of normal saline for 5 to 10 minutes. Patients were categorized as OPVH if PWP increased to >15 mm Hg after fluid challenge. Baseline hemodynamics in 207 patients met criteria for PAH. After fluid challenge, 46 patients (22.2%) developed a PWP>15 mm Hg and were reclassified as OPVH. Patients with OPVH had a greater increase in PWP compared with patients with PAH, P<0.001, and their demographics and comorbid illnesses were similar to patients with PVH. There were no adverse events related to fluid challenge.
Conclusions: Fluid challenge at the time of right heart catheterization is easily performed, safe, and identifies a large group of patients diagnosed initially with PAH, but for whom OPVH contributes to pulmonary hypertension. These results have implications for therapeutic trials in PAH and support the routine use of fluid challenge during right heart catheterization in patients with risk factors for PVH.
Keywords: hemodynamics; hypertension, pulmonary; pulmonary arterial hypertension; pulmonary heart disease.
Figures
Comment in
-
Invasive assessment of pulmonary hypertension: time for a more fluid approach?Circ Heart Fail. 2014 Jan;7(1):2-4. doi: 10.1161/CIRCHEARTFAILURE.113.000983. Circ Heart Fail. 2014. PMID: 24449809 No abstract available.
References
-
- Hatano S, Strasser T, editors. Primary Pulmonary Hypertension: Report on a WHO Meeting. World Health Organization; Geneva: 1975. pp. 7–45. Figure Legends.
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–S54. - PubMed
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G, ESC Committee for Practice Guidelines (CPG) Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009;30:2493–2537. - PubMed
-
- Califf RM, Adams KF, McKenna WJ, Gheorghiade M, Uretsky BF, McNulty SE, Darius H, Schulman K, Zannad F, Handberg-Thurmond E, Harrell FE, Jr, Wheeler W, Soler-Soler J, Swedberg K. A randomized controlled trial of epoprostenol therapy for severe congestive heart failure: the Flolan International Randomized Survival Trial (FIRST). Am Heart J. 1997;134:44–54. - PubMed
-
- Anand I, McMurray J, Cohn JN, Konstam MA, Notter T, Quitzau K, Ruschitzka F, Lüscher TF, EARTH investigators Long-term effects of darusentan on left ventricular remodeling and clinical outcomes in endothelin receptor antagonist trial in heart failure (EARTH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:347–354. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
