

Review
doi: 10.1111/bju.12593.
Epub 2014 May 22.
Current status of magnetic resonance imaging (MRI) and ultrasonography fusion software platforms for guidance of prostate biopsies
Affiliations
- PMID: 24298917
- PMCID: PMC4568118
- DOI: 10.1111/bju.12593
Item in Clipboard
Review
Current status of magnetic resonance imaging (MRI) and ultrasonography fusion software platforms for guidance of prostate biopsies
BJU Int.
2014 Nov.
Abstract
Prostate MRI is currently the best diagnostic imaging method for detecting PCa. Magnetic resonance imaging (MRI)/ultrasonography (US) fusion allows the sensitivity and specificity of MRI to be combined with the real-time capabilities of transrectal ultrasonography (TRUS). Multiple approaches and techniques exist for MRI/US fusion and include direct 'in bore' MRI biopsies, cognitive fusion, and MRI/US fusion via software-based image coregistration platforms.
Keywords: MRI/US fusion; MRI/US fusion platforms; prostate MRI; targeted biopsy.
© 2013 The Authors. BJU International © 2013 BJU International.
Figures
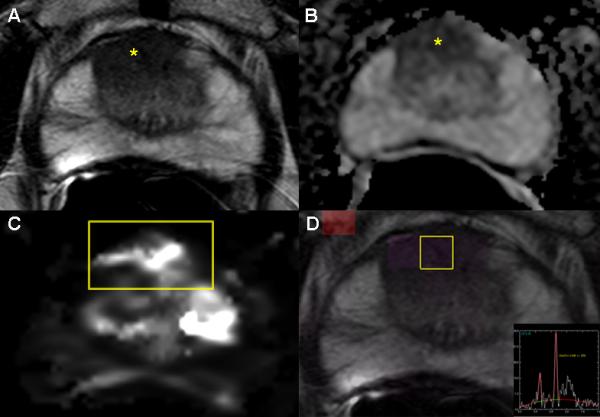
Images from a 65 year old male with serum PSA 8.7 ng/mL and four previously
negative TRUS biopsies who underwent a multiparametric MRI(mpMRI).The axial T2W
MR image (A) demonstrates an anterior hypointense lesion in the right apical
central gland (yellow asterisk); an ADC map of DW-MRI (B) shows a hypointense
focus (yellow asterisk) indicating restricted diffusion; quantitative mapping
from DCE-MRI (C) localizes the tumor(yellow box); and MRSI (D) (yellow box)
demonstrates an increased choline-to-citrine ratio within the lesion. This
patient underwent a MRI/US fusion-guided biopsy following mpMRI demonstrating
Gleason 4+4 = 8 (90% in 2 targeted cores) in the right anterior lesion.
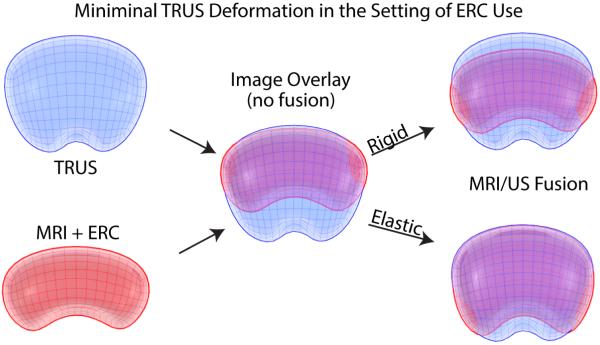
Elastic and Rigid Software Image Registration Methods. Pre-biopsy MR data is
registered with real-time TRUS images by aligning landmarks(e.g. points, curves,
surfaces,) in corresponding images via rigid or elastic transformations. (A)
represents MRI/US registration when there is minimal TRUS deformation and use of
an endorectal coil (ERC) for MR images, and (B) demonstrates increased manual
TRUS deformation that can mimic ERC deformation. As seen above, a simple overlay
of TRUS and MRI models (middle images in panels A and B) results in reduced
correlation between imaging modalities. A rigid registration method can account
for translational and rotational differences between models while an elastic
registration method has the additional ability to account for local deformations
(e.g. caused by an endorectal coil or TRUS probe). However, elastic warping can
move or alter relative anatomic location despite more matched borders. ERC,
endorectal coil.
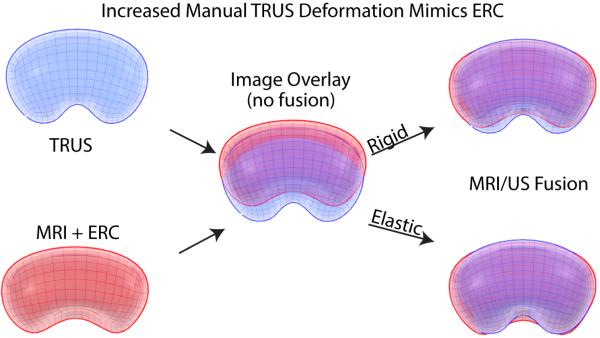
Elastic and Rigid Software Image Registration Methods. Pre-biopsy MR data is
registered with real-time TRUS images by aligning landmarks(e.g. points, curves,
surfaces,) in corresponding images via rigid or elastic transformations. (A)
represents MRI/US registration when there is minimal TRUS deformation and use of
an endorectal coil (ERC) for MR images, and (B) demonstrates increased manual
TRUS deformation that can mimic ERC deformation. As seen above, a simple overlay
of TRUS and MRI models (middle images in panels A and B) results in reduced
correlation between imaging modalities. A rigid registration method can account
for translational and rotational differences between models while an elastic
registration method has the additional ability to account for local deformations
(e.g. caused by an endorectal coil or TRUS probe). However, elastic warping can
move or alter relative anatomic location despite more matched borders. ERC,
endorectal coil.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011 Mar-Apr;61:69–90. 2011. - PubMed
-
- Krahn MD, Mahoney JE, Eckman MH, Trachtenberg J, Pauker SG, Detsky AS. Screening for prostate cancer. A decision analytic view. JAMA. 1994 Sep;272:773–80. - PubMed
-
- Chodak GW KP, Schoenberg HW. Assessment of screening for prostate cancer using the digital rectal examination. J Urol. 1989;141(5):1136. - PubMed
-
- Newcomer LM, Stanford JL, Blumenstein BA, Brawer MK. Temporal trends in rates of prostate cancer: declining incidence of advanced stage disease, 1974 to 1994. J Urol. 1997 Oct;158:1427–30. - PubMed
-
- Hodge KK, McNeal JE, Stamey TA. Ultrasound guided transrectal core biopsies of the palpably abnormal prostate. J Urol. 1989 Jul;142:66–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
