

Early effects of parathyroid hormone on bisphosphonate/steroid-associated compromised osseous wound healing
- PMID: 24301537
- PMCID: PMC3923117
- DOI: 10.1007/s00198-013-2570-8
Early effects of parathyroid hormone on bisphosphonate/steroid-associated compromised osseous wound healing
Abstract
Summary: Administration of intermittent parathyroid hormone (PTH) promoted healing of tibial osseous defects and tooth extraction wounds and prevented the development of necrotic lesions in rats on a combined bisphosphonate and steroid regimen.
Introduction: Osteonecrosis of the jaw (ONJ) has emerged in association with antiresorptive therapies. The pathophysiology of ONJ is unknown and no established cure currently exists. Our objective was to determine the effect of intermittent PTH administration on early osseous healing in the jaw and long bones of rats receiving bisphosphonate and steroid treatment.
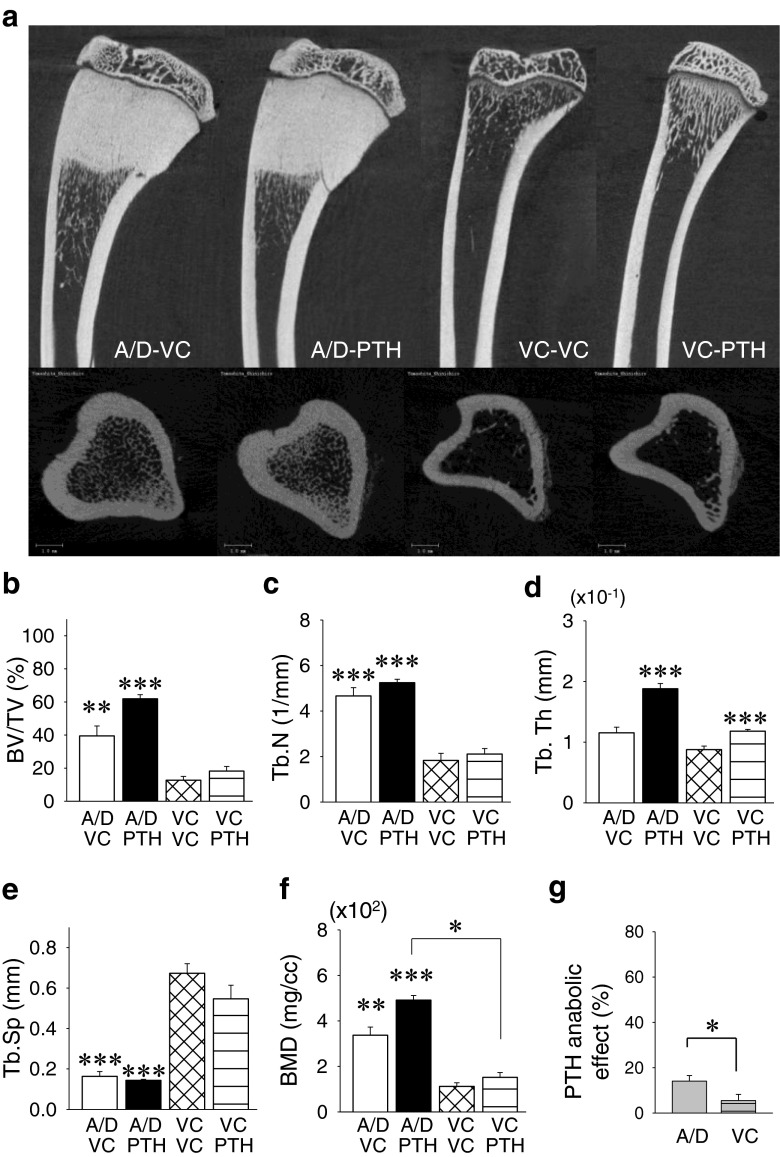
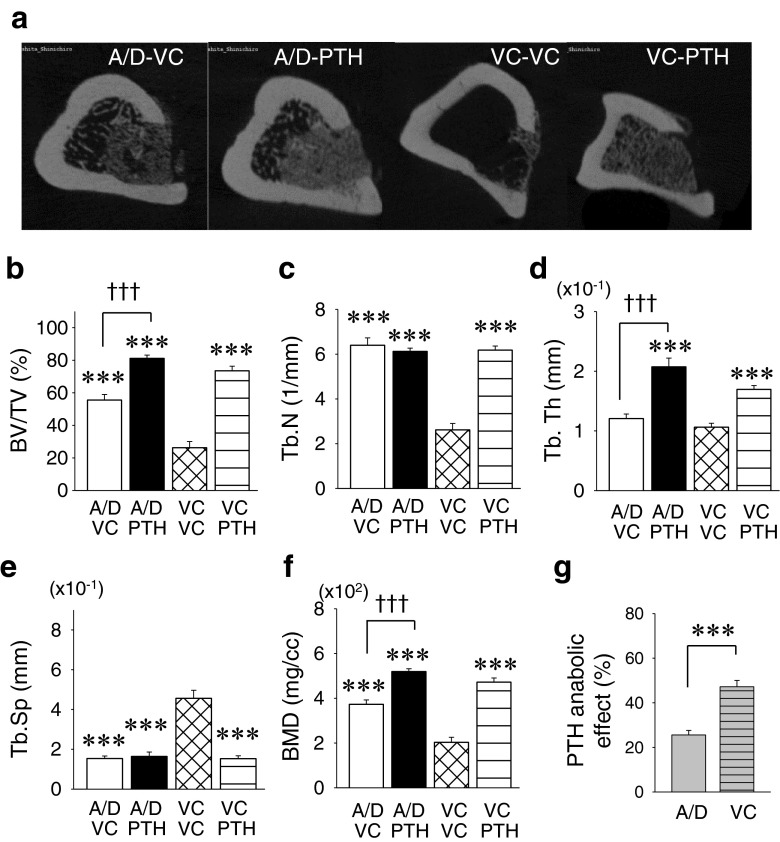
Methods: Ovariectomized rats received the combination therapy of alendronate and dexamethasone (ALN/DEX) for 12 weeks. Osseous wounds were created in the jaw and tibia. PTH was administered intermittently and healing at 2 weeks post-op was compared between the jaw and tibia by microcomputed tomography and histomorphometric analyses.
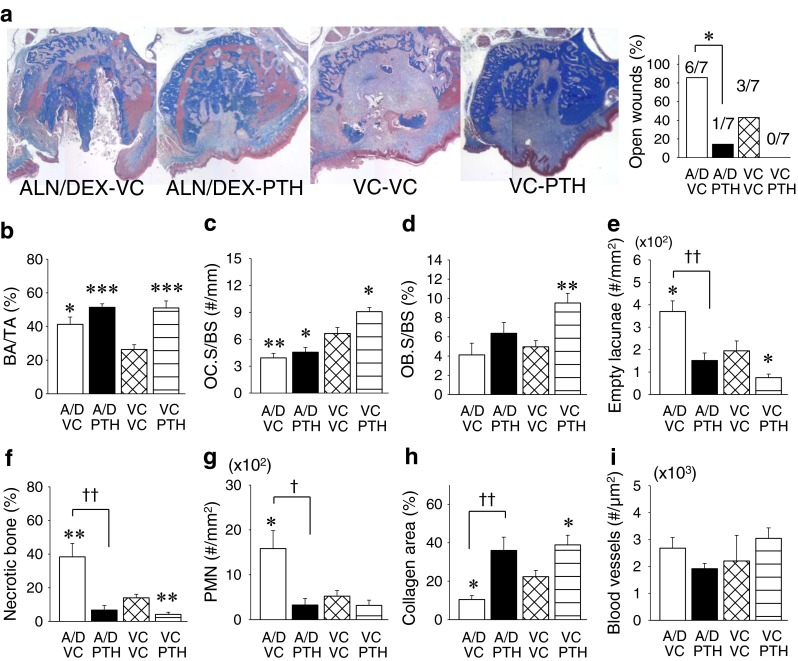
Results: ALN/DEX treatment was associated with necrotic open wounds in the jaw but had no negative effects on healing and promoted bone fill in tibial defects. PTH therapy prevented the development of necrotic lesions in the jaw and promoted healing of the tibial defects. PTH therapy was associated with the promotion of osteocyte survival in osseous wounds both in the jaw and tibia.
Conclusions: Wound healing was impaired in the jaw in rats on a combined bisphosphonate and steroid regimen, and PTH therapy rescued necrotic lesions. These findings suggest that PTH therapy could be utilized to prevent ONJ from occurring in patients on combination antiresorptive and steroid therapy.
Figures



Similar articles
-
Bisphosphonate-induced osteonecrosis of the jaw in a rat model arises first after the bone has become exposed. No primary necrosis in unexposed bone.J Oral Pathol Med. 2012 Jul;41(6):494-9. doi: 10.1111/j.1600-0714.2011.01125.x. Epub 2012 Jan 23. J Oral Pathol Med. 2012. PMID: 22268631
-
Distinctive tooth-extraction socket healing: bisphosphonate versus parathyroid hormone therapy.J Periodontol. 2014 Jan;85(1):24-33. doi: 10.1902/jop.2013.130094. Epub 2013 May 20. J Periodontol. 2014. PMID: 23688101 Free PMC article.
-
Differential modulation of zoledronate and etidronate in osseous healing of an extracted socket and tibia defect.Oral Surg Oral Med Oral Pathol Oral Radiol. 2017 Jan;123(1):8-19. doi: 10.1016/j.oooo.2016.08.009. Epub 2016 Aug 18. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017. PMID: 27727104
-
Parathyroid hormone applications in the craniofacial skeleton.J Dent Res. 2013 Jan;92(1):18-25. doi: 10.1177/0022034512464779. Epub 2012 Oct 15. J Dent Res. 2013. PMID: 23071071 Free PMC article. Review.
-
The effects of bisphosphonates on jaw bone remodeling, tissue properties, and extraction healing.Odontology. 2011 Jan;99(1):8-17. doi: 10.1007/s10266-010-0153-0. Epub 2011 Jan 27. Odontology. 2011. PMID: 21271320 Review.
Cited by
-
Mouse anti-RANKL antibody delays oral wound healing and increases TRAP-positive mononuclear cells in bone marrow.Clin Oral Investig. 2016 May;20(4):727-36. doi: 10.1007/s00784-015-1550-0. Epub 2015 Aug 9. Clin Oral Investig. 2016. PMID: 26254598 Free PMC article.
-
Intramedullary injury combined with osteoporosis therapeutics regulates targeted local osteogenesis.Sci Rep. 2021 Jan 12;11(1):205. doi: 10.1038/s41598-020-80316-y. Sci Rep. 2021. PMID: 33436871 Free PMC article.
-
Preclinical models of medication-related osteonecrosis of the jaw (MRONJ).Bone. 2021 Dec;153:116184. doi: 10.1016/j.bone.2021.116184. Epub 2021 Sep 11. Bone. 2021. PMID: 34520898 Free PMC article. Review.
-
Effect of intermittent teriparatide (PTH 1-34) on the alveolar healing process in orchiectomized rats.Clin Oral Investig. 2019 May;23(5):2313-2322. doi: 10.1007/s00784-018-2672-y. Epub 2018 Oct 6. Clin Oral Investig. 2019. PMID: 30291494
-
Effect of Alendronate on Bone Formation during Tooth Extraction Wound Healing.J Dent Res. 2015 Sep;94(9):1251-8. doi: 10.1177/0022034515592867. Epub 2015 Jun 29. J Dent Res. 2015. PMID: 26124220 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
