

Effect of communication skills training for residents and nurse practitioners on quality of communication with patients with serious illness: a randomized trial
- PMID: 24302090
- PMCID: PMC4310457
- DOI: 10.1001/jama.2013.282081
Effect of communication skills training for residents and nurse practitioners on quality of communication with patients with serious illness: a randomized trial
Erratum in
- JAMA. 2014 Apr 2;311(13):1360
Abstract
Importance: Communication about end-of-life care is a core clinical skill. Simulation-based training improves skill acquisition, but effects on patient-reported outcomes are unknown.
Objective: To assess the effects of a communication skills intervention for internal medicine and nurse practitioner trainees on patient- and family-reported outcomes.
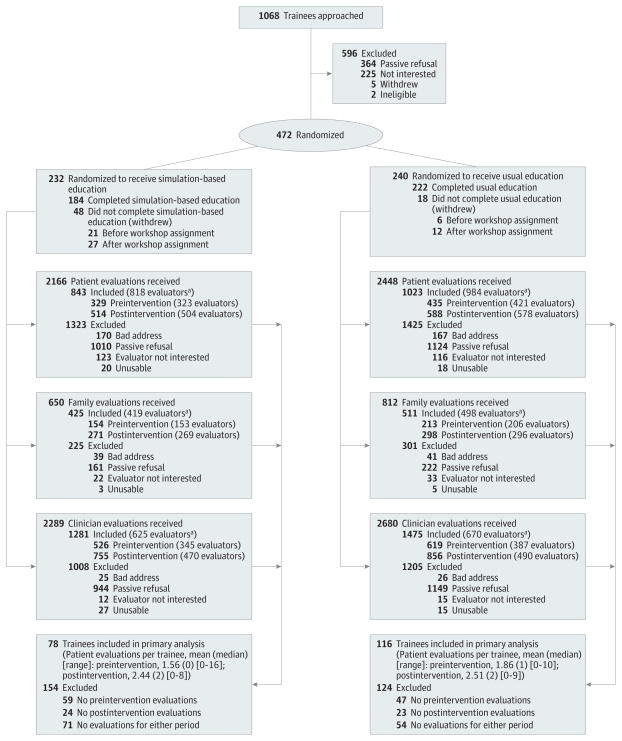
Design, setting, and participants: Randomized trial conducted with 391 internal medicine and 81 nurse practitioner trainees between 2007 and 2013 at the University of Washington and Medical University of South Carolina.
Intervention: Participants were randomized to an 8-session, simulation-based, communication skills intervention (N = 232) or usual education (N = 240).
Main outcomes and measures: Primary outcome was patient-reported quality of communication (QOC; mean rating of 17 items rated from 0-10, with 0 = poor and 10 = perfect). Secondary outcomes were patient-reported quality of end-of-life care (QEOLC; mean rating of 26 items rated from 0-10) and depressive symptoms (assessed using the 8-item Personal Health Questionnaire [PHQ-8]; range, 0-24, higher scores worse) and family-reported QOC and QEOLC. Analyses were clustered by trainee.
Results: There were 1866 patient ratings (44% response) and 936 family ratings (68% response). The intervention was not associated with significant changes in QOC or QEOLC. Mean values for postintervention patient QOC and QEOLC were 6.5 (95% CI, 6.2 to 6.8) and 8.3 (95% CI, 8.1 to 8.5) respectively, compared with 6.3 (95% CI, 6.2 to 6.5) and 8.3 (95% CI, 8.1 to 8.4) for control conditions. After adjustment, comparing intervention with control, there was no significant difference in the QOC score for patients (difference, 0.4 points [95% CI, -0.1 to 0.9]; P = .15) or families (difference, 0.1 [95% CI, -0.8 to 1.0]; P = .81). There was no significant difference in QEOLC score for patients (difference, 0.3 points [95% CI, -0.3 to 0.8]; P = .34) or families (difference, 0.1 [95% CI, -0.7 to 0.8]; P = .88). The intervention was associated with significantly increased depression scores among patients of postintervention trainees (mean score, 10.0 [95% CI, 9.1 to 10.8], compared with 8.8 [95% CI, 8.4 to 9.2]) for control conditions; adjusted model showed an intervention effect of 2.2 (95% CI, 0.6 to 3.8; P = .006).
Conclusions and relevance: Among internal medicine and nurse practitioner trainees, simulation-based communication training compared with usual education did not improve quality of communication about end-of-life care or quality of end-of-life care but was associated with a small increase in patients' depressive symptoms. These findings raise questions about skills transfer from simulation training to actual patient care and the adequacy of communication skills assessment.
Trial registration: clinicaltrials.gov Identifier: NCT00687349.
Conflict of interest statement
Figures
Comment in
-
Improving communication with patients: learning by doing.JAMA. 2013 Dec 4;310(21):2257-8. doi: 10.1001/jama.2013.281828. JAMA. 2013. PMID: 24302087 No abstract available.
-
Effect of communication training on patient, family and healthcare provider outcomes: missing links.Evid Based Med. 2014 Aug;19(4):158. doi: 10.1136/eb-2014-101720. Epub 2014 Feb 7. Evid Based Med. 2014. PMID: 24510480 No abstract available.
-
Training for effective patient communication.JAMA. 2014 Apr 2;311(13):1355. doi: 10.1001/jama.2014.1757. JAMA. 2014. PMID: 24691613 No abstract available.
-
Training for effective patient communication.JAMA. 2014 Apr 2;311(13):1355-6. doi: 10.1001/jama.2014.1763. JAMA. 2014. PMID: 24691614 No abstract available.
-
Training for effective patient communication.JAMA. 2014 Apr 2;311(13):1356. doi: 10.1001/jama.2014.1766. JAMA. 2014. PMID: 24691615 No abstract available.
-
Training for effective patient communication--reply.JAMA. 2014 Apr 2;311(13):1356-7. doi: 10.1001/jama.2014.1475. JAMA. 2014. PMID: 24691616 No abstract available.
References
-
- Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733–742. - PubMed
-
- Greer JA, Pirl WF, Jackson VA, et al. Effect of early palliative care on chemotherapy use and end-of-life care in patients with metastatic non-small-cell lung cancer. J Clin Oncol. 2012;30(4):394–400. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
