

Left atrial structure and function in atrial fibrillation: ENGAGE AF-TIMI 48
- PMID: 24302269
- PMCID: PMC4048534
- DOI: 10.1093/eurheartj/eht500
Left atrial structure and function in atrial fibrillation: ENGAGE AF-TIMI 48
Abstract
Aims: The complex relationship between left atrial (LA) structure and function, electrical burden of atrial fibrillation (AF) and stroke risk is not well understood. We aimed to describe LA structure and function in AF.
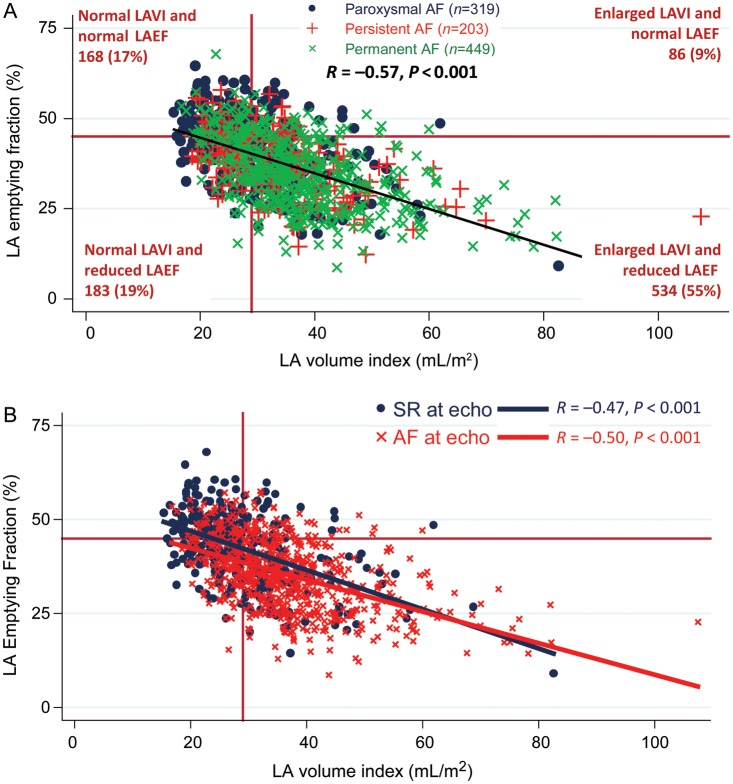
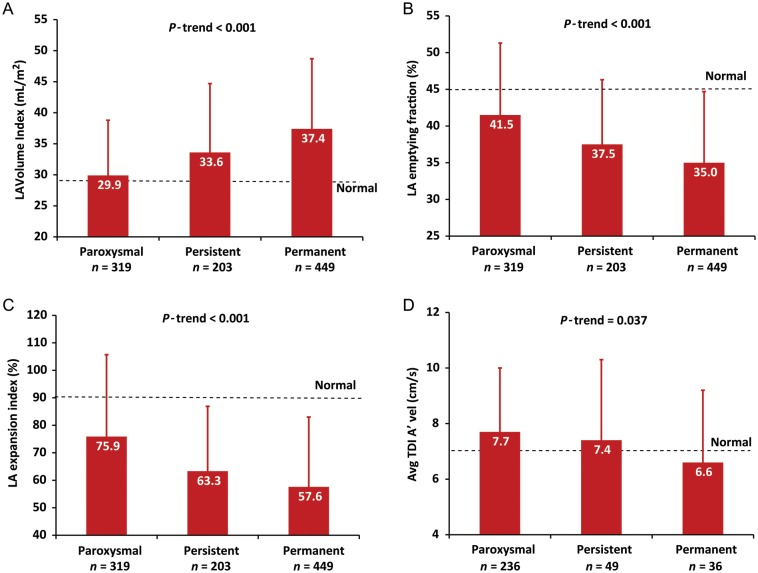
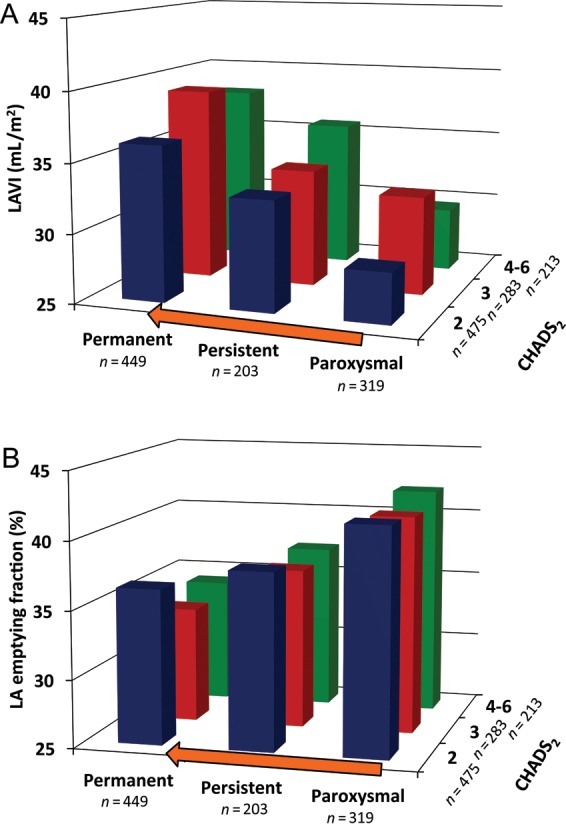
Methods and results: Left atrial structure and function was assessed in 971 subjects enrolled in the echocardiographic substudy of ENGAGE AF-TIMI 48. Left atrial size, emptying fraction (LAEF), and contractile function were compared across AF types (paroxysmal, persistent, or permanent) and CHADS2 scores as an estimate of stroke risk. The majority of AF patients (55%) had both LA enlargement and reduced LAEF, with an inverse relationship between LA size and LAEF (R = -0.57, P < 0.001). With an increasing electrical burden of AF and higher CHADS2 scores, LA size increased and LAEF declined. Moreover, 19% of AF subjects had impaired LAEF despite normal LA size, and LA contractile dysfunction was present even among the subset of AF subjects in sinus rhythm at the time of echocardiography.
Conclusions: In a contemporary AF population, LA structure and function were increasingly abnormal with a greater electrical burden of AF and higher stroke risk estimated by the CHADS2 score. Moreover, LA dysfunction was present despite normal LA size and sinus rhythm, suggesting that the assessment of LA function may add important incremental information in the evaluation of AF patients.
Clinical trial registration: http://www.clinicaltrials.gov; ID = NCT00781391.
Keywords: Atrial fibrillation; ENGAGE AF-TIMI 48; Echocardiography; Left atrium; Stroke.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2013. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Dittrich HC, Pearce LA, Asinger RW, McBride R, Webel R, Zabalgoitia M, Pennock GD, Safford RE, Rothbart RM, Halperin JL, Hart RG. Left atrial diameter in nonvalvular atrial fibrillation: an echocardiographic study. Stroke Prevention in Atrial Fibrillation Investigators. Am Heart J. 1999;137:494–499. doi: 10.1016/S0002-8703(99)70498-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
