

Medical interventions for traumatic hyphema
- PMID: 24302299
- PMCID: PMC4268787
- DOI: 10.1002/14651858.CD005431.pub3
Medical interventions for traumatic hyphema
Update in
-
Medical interventions for traumatic hyphema.Cochrane Database Syst Rev. 2019 Jan 14;1(1):CD005431. doi: 10.1002/14651858.CD005431.pub4. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2023 Mar 13;3:CD005431. doi: 10.1002/14651858.CD005431.pub5. PMID: 30640411 Free PMC article. Updated.
Abstract
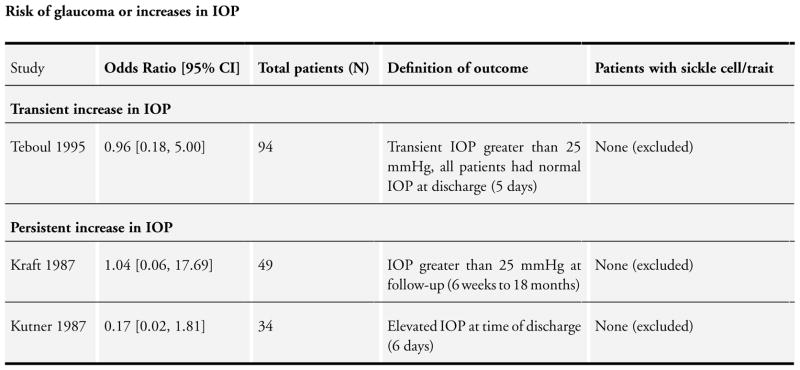
Background: Traumatic hyphema is the entry of blood into the anterior chamber (the space between the cornea and iris) subsequent to a blow or a projectile striking the eye. Hyphema uncommonly causes permanent loss of vision. Associated trauma (e.g. corneal staining, traumatic cataract, angle recession glaucoma, optic atrophy, etc.) may seriously affect vision. Such complications may lead to permanent impairment of vision. Patients with sickle cell trait/disease may be particularly susceptible to increases of elevated intraocular pressure. If rebleeding occurs, the rates and severity of complications increase.
Objectives: To assess the effectiveness of various medical interventions in the management of traumatic hyphema.
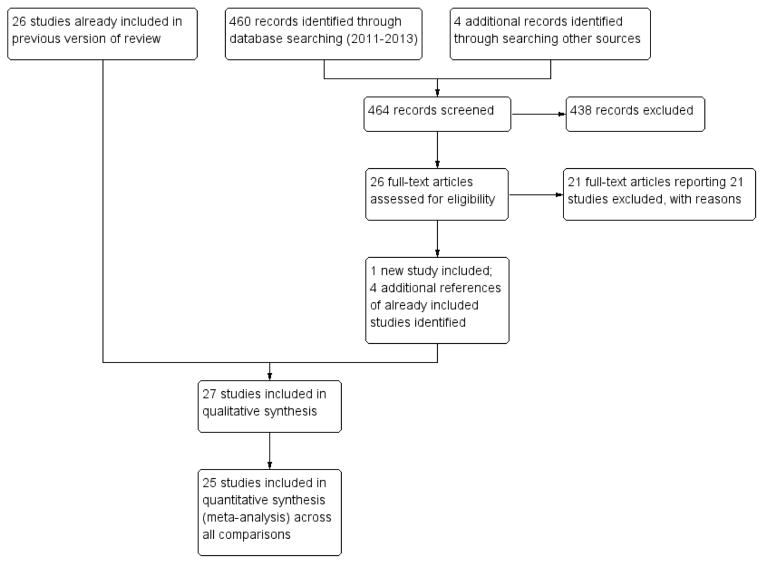
Search methods: We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2013, Issue 8), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE (January 1946 to August 2013), EMBASE (January 1980 to August 2013), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We last searched the electronic databases on 30 August 2013.
Selection criteria: Two authors independently assessed the titles and abstracts of all reports identified by the electronic and manual searches. In this review, we included randomized and quasi-randomized trials that compared various medical interventions versus other medical interventions or control groups for the treatment of traumatic hyphema following closed globe trauma. We applied no restrictions regarding age, gender, severity of the closed globe trauma, or level of visual acuity at the time of enrolment.
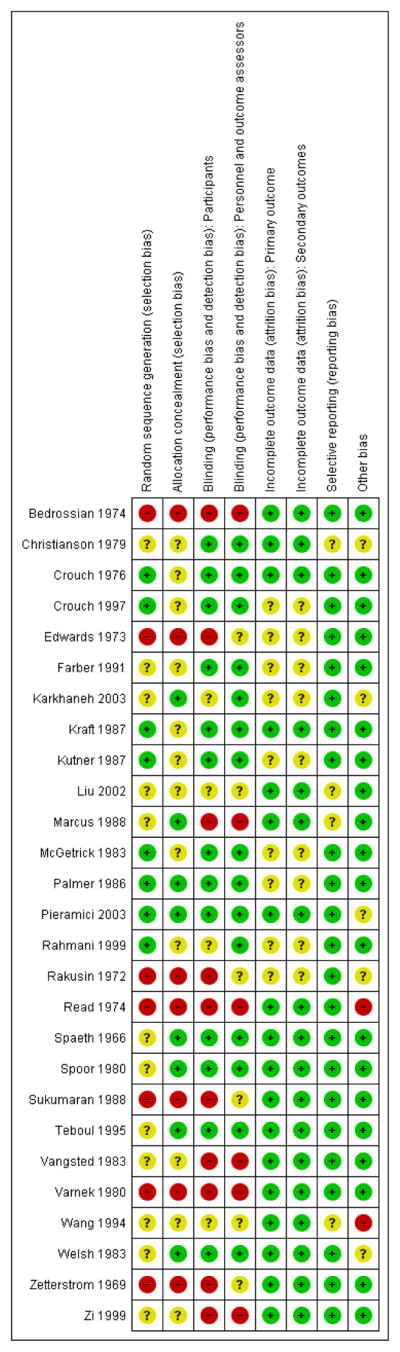
Data collection and analysis: Two authors independently extracted the data for the primary and secondary outcomes. We entered and analyzed data using Review Manager 5. We performed meta-analyses using a fixed-effect model and reported dichotomous outcomes as odds ratios and continuous outcomes as mean differences.
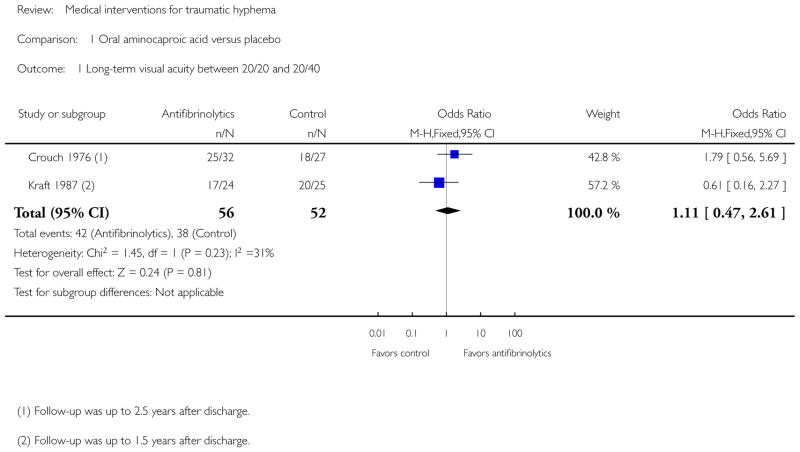
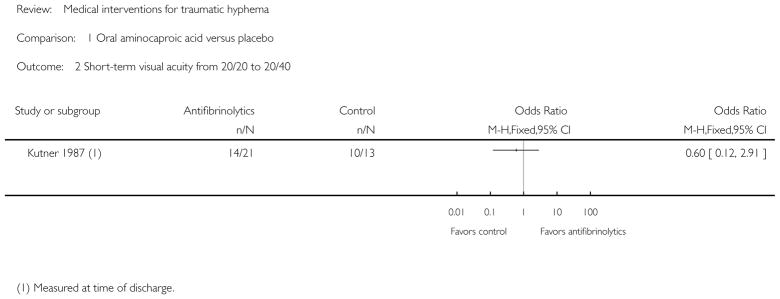
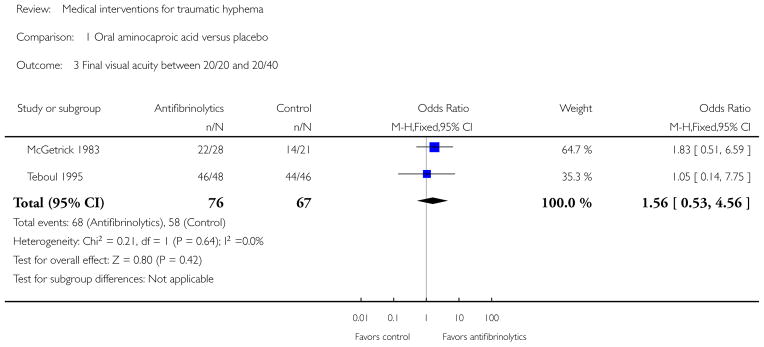
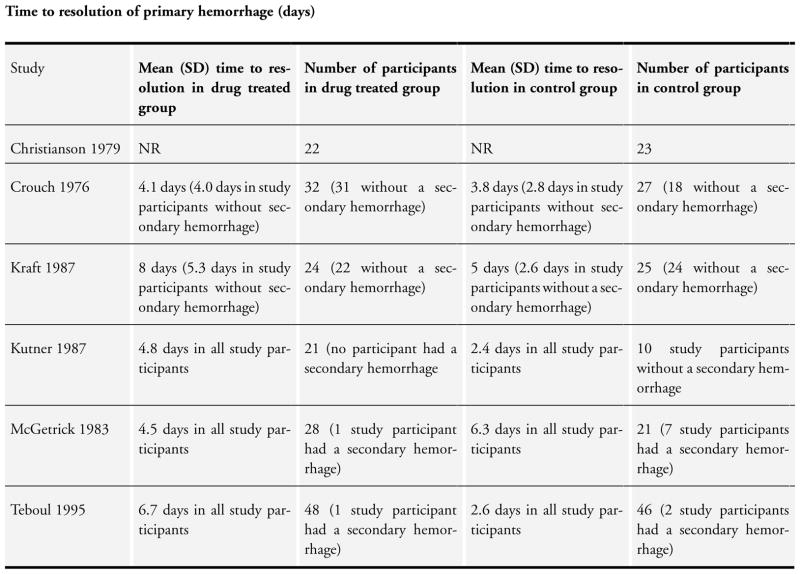
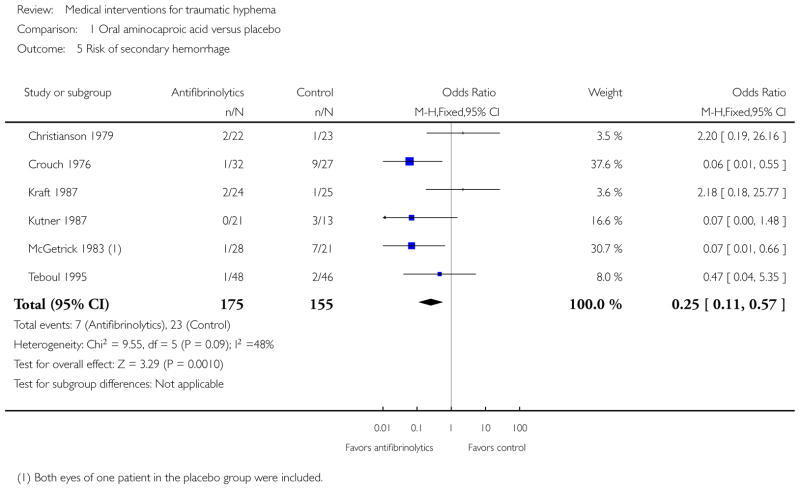
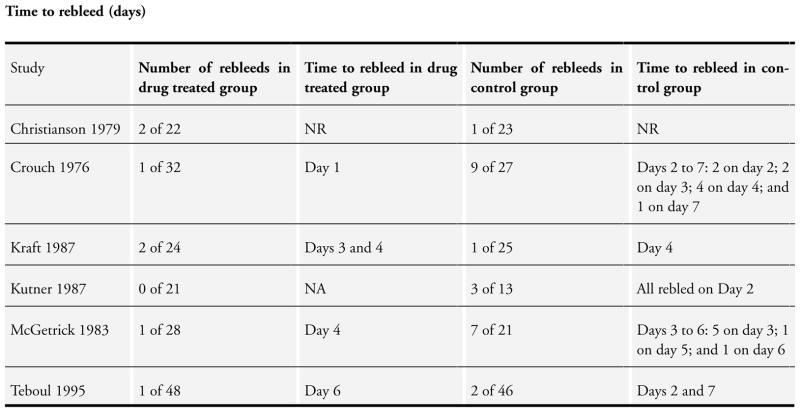
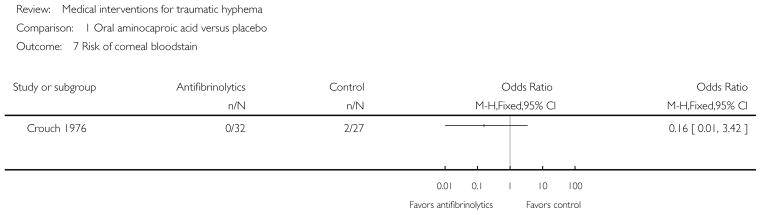
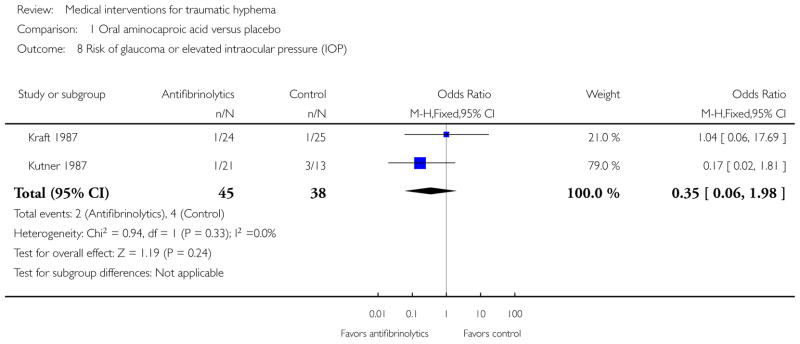
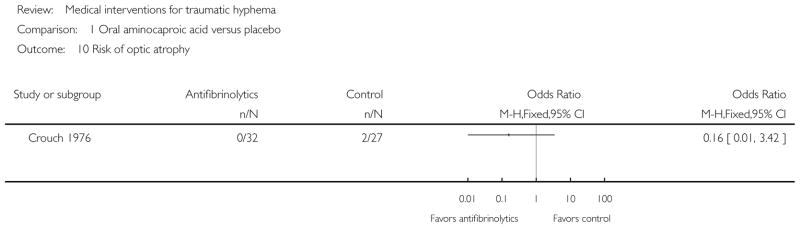
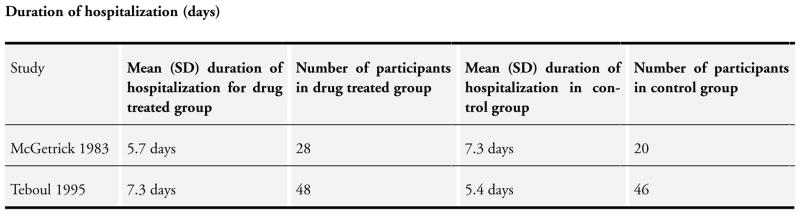
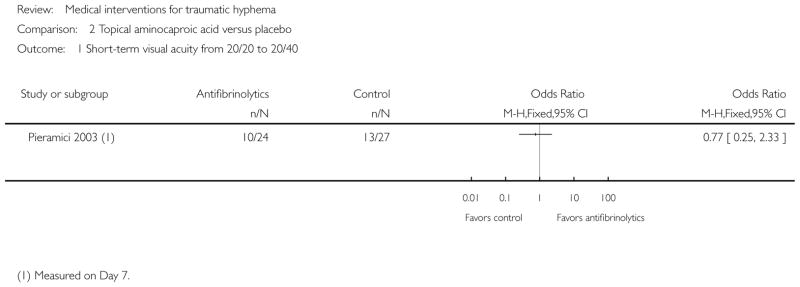
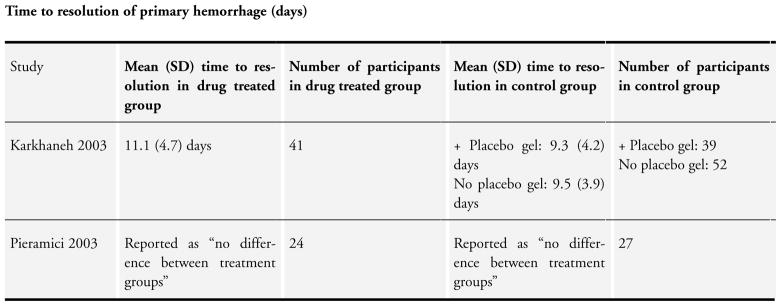
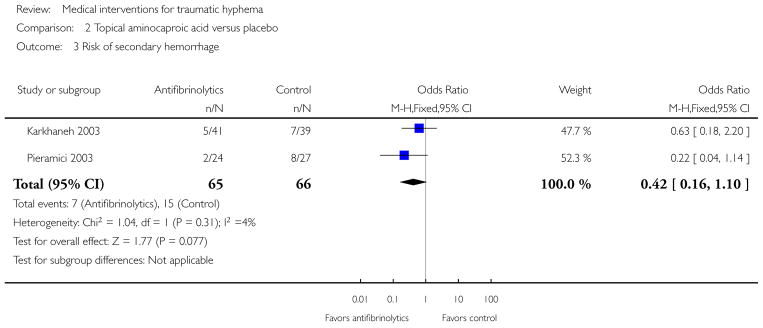
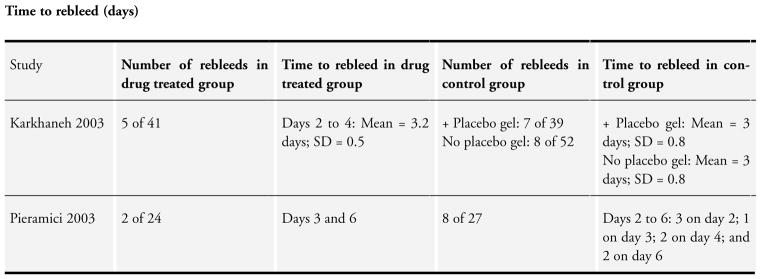
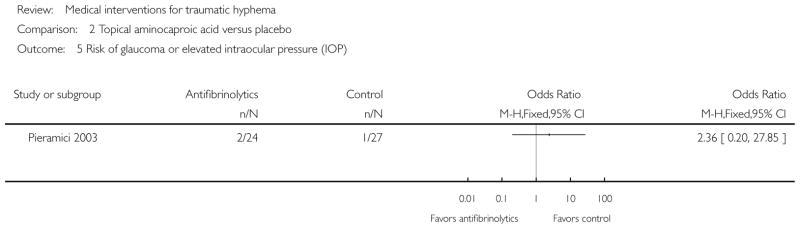
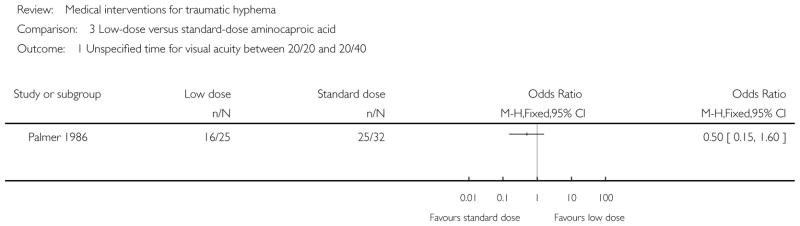
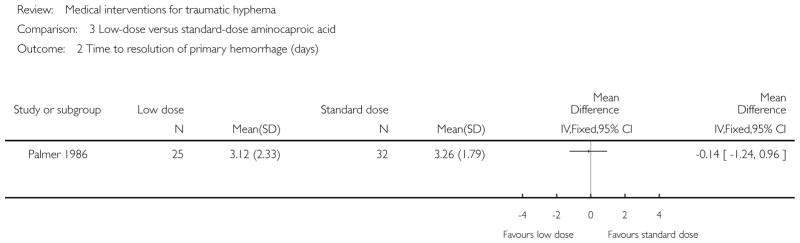
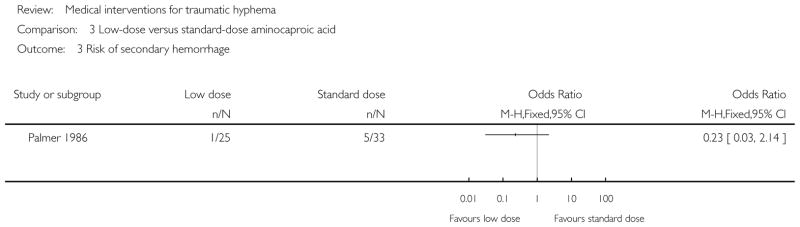
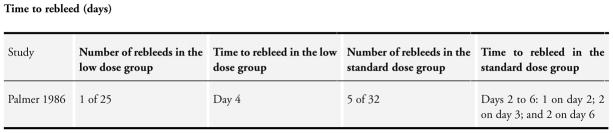
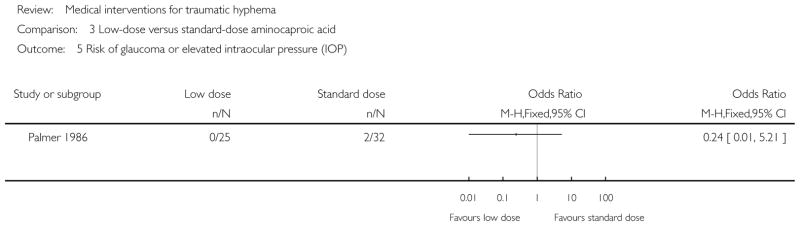
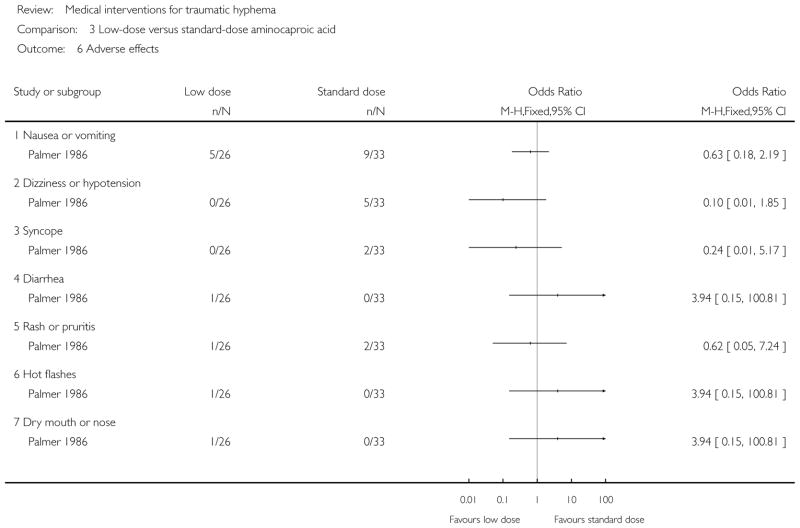
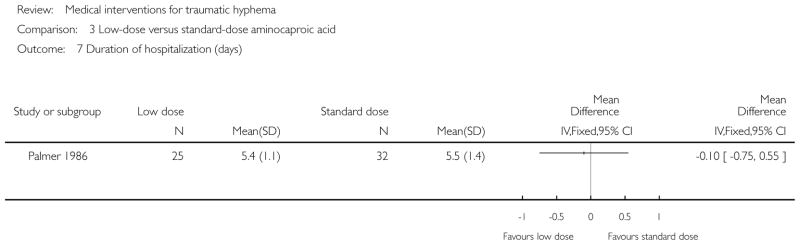
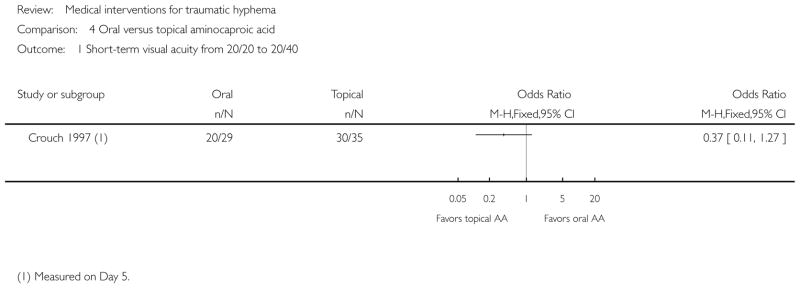
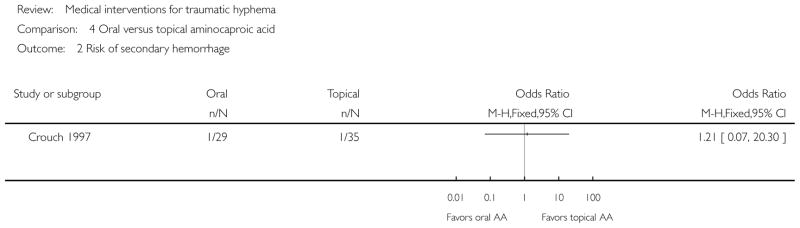
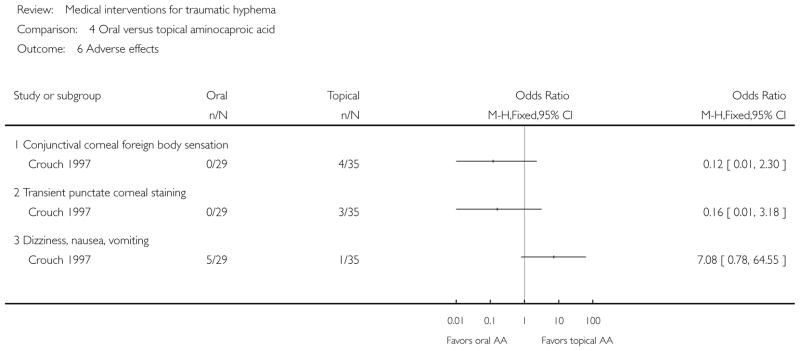
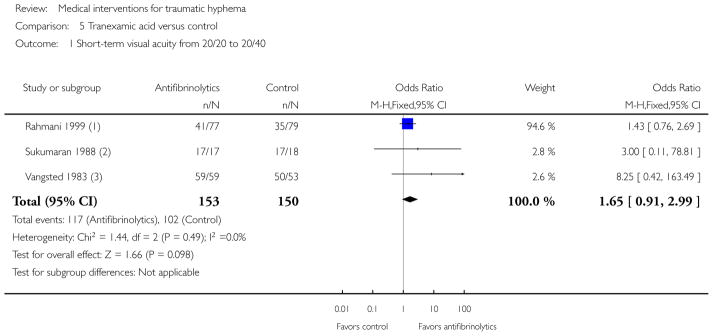
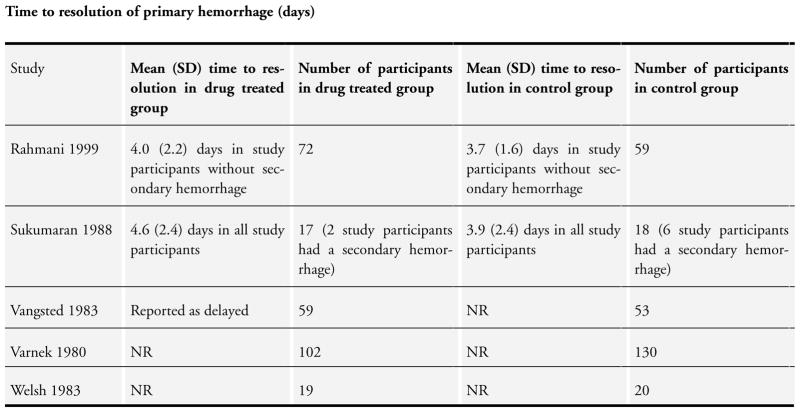
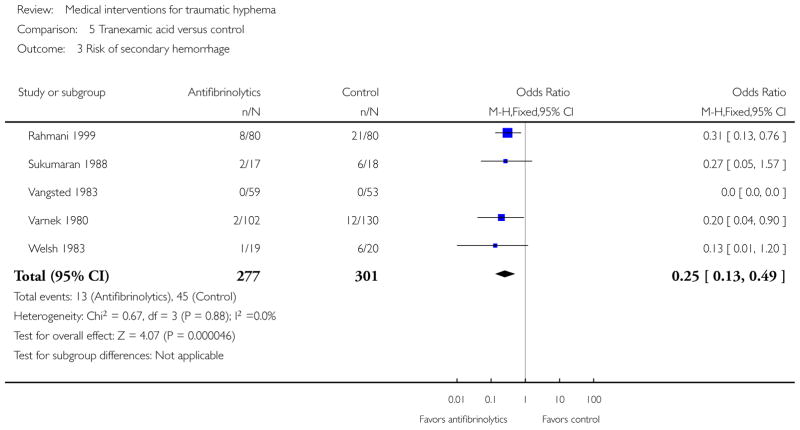
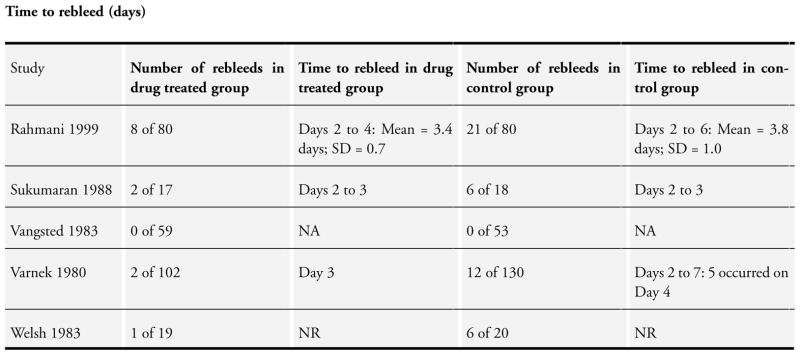
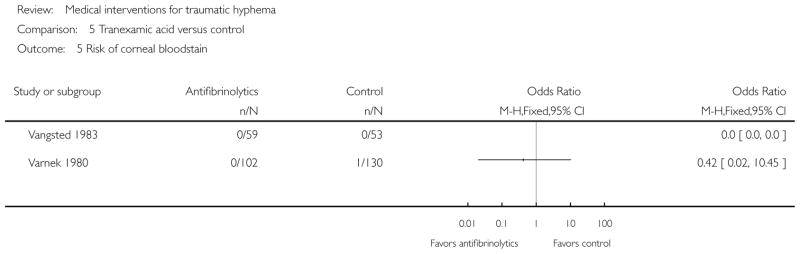
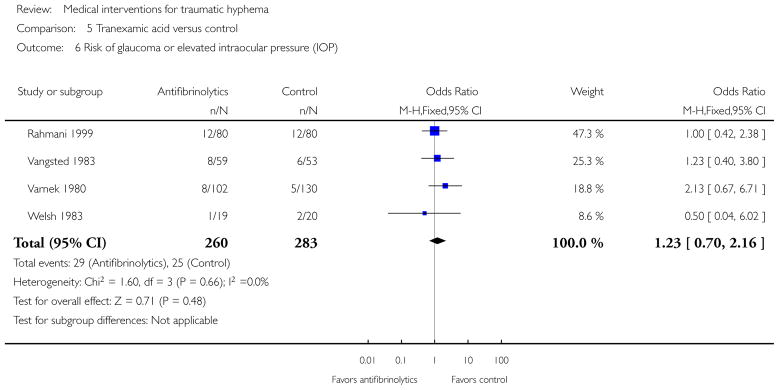
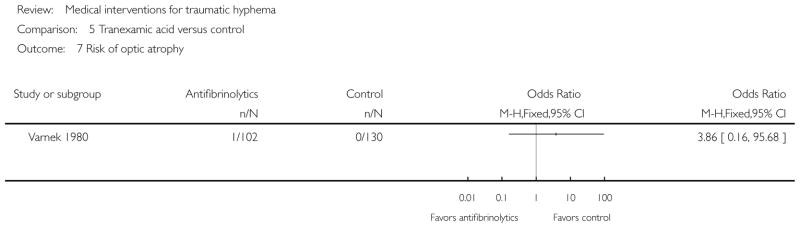
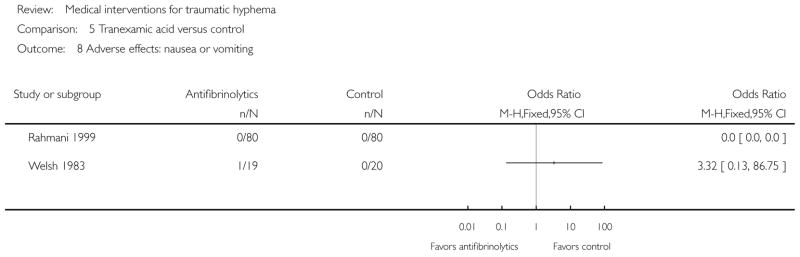
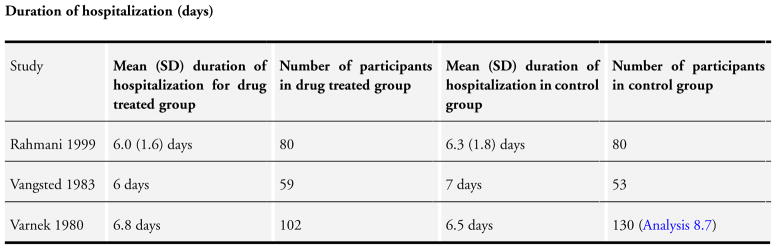
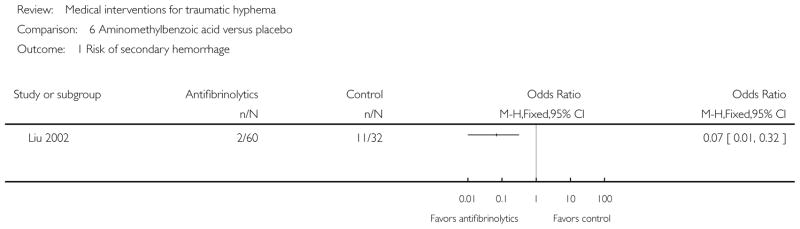
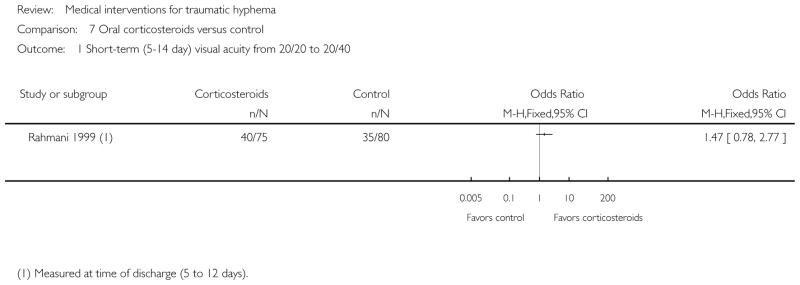
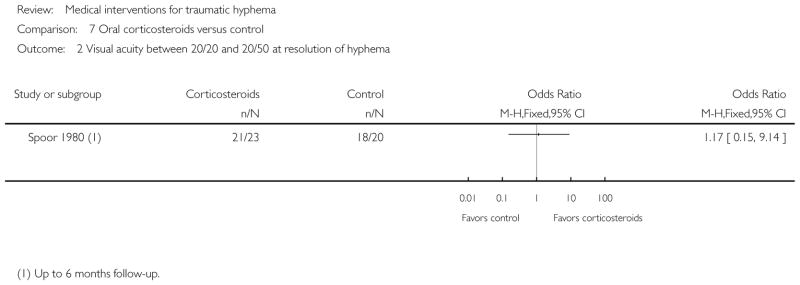
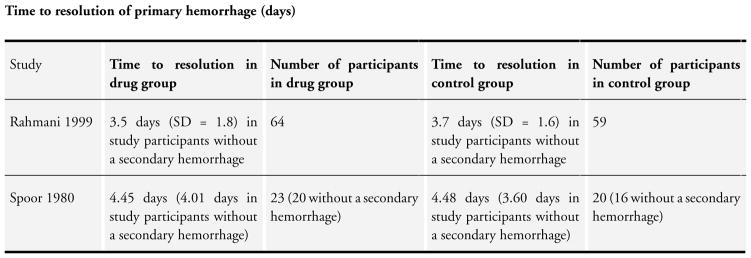
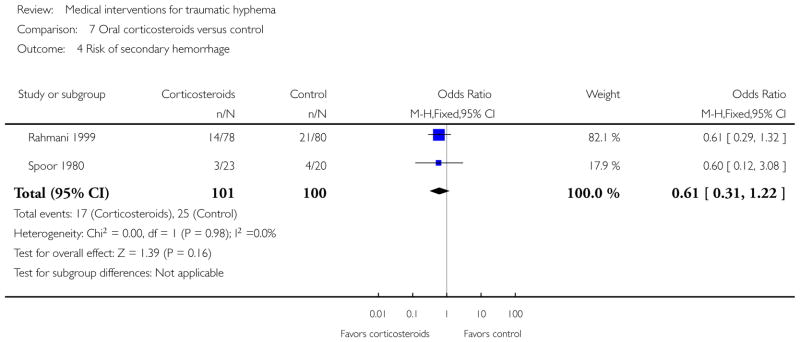
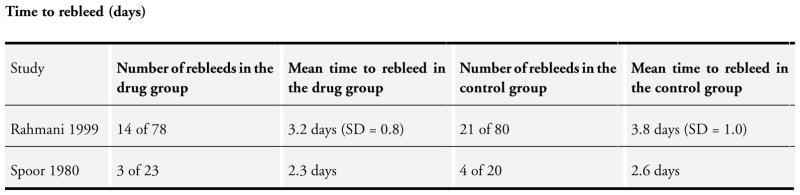
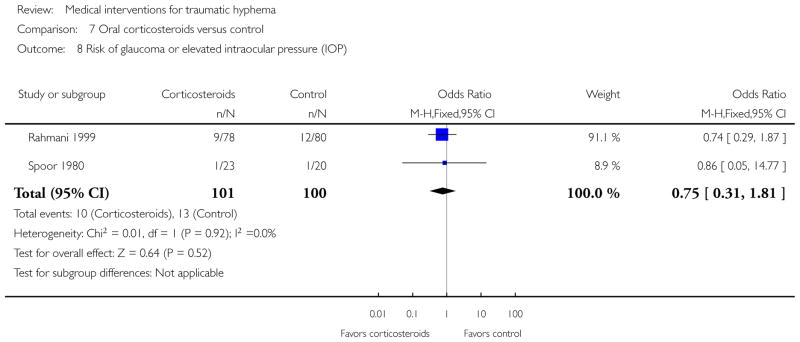
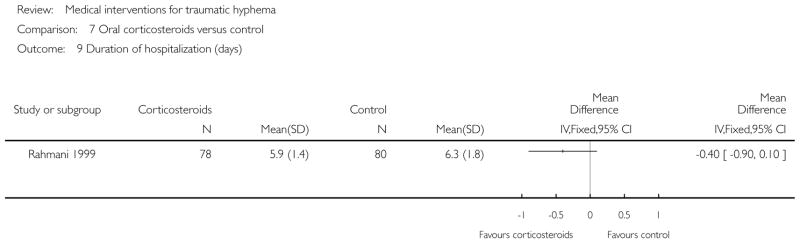
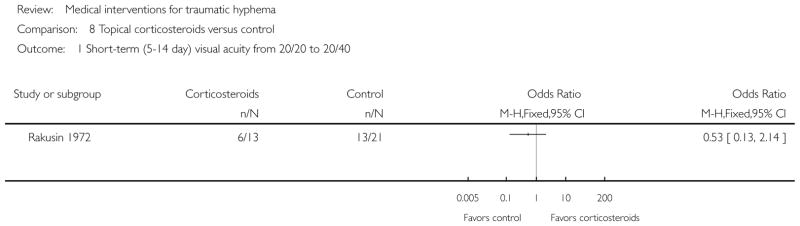
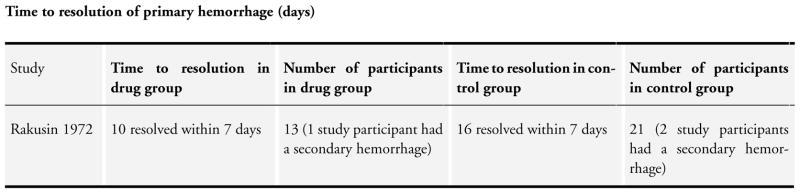
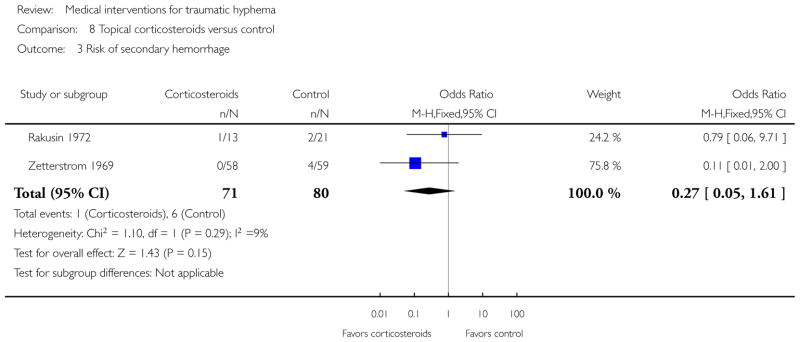
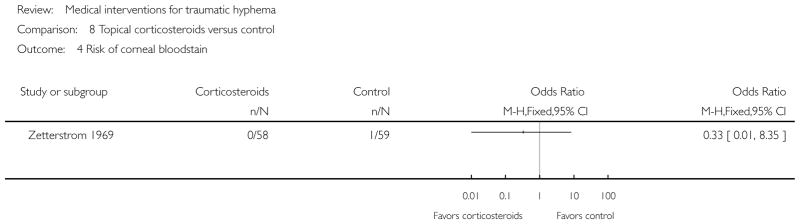
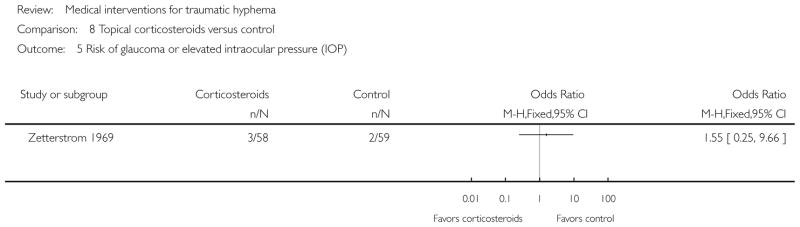
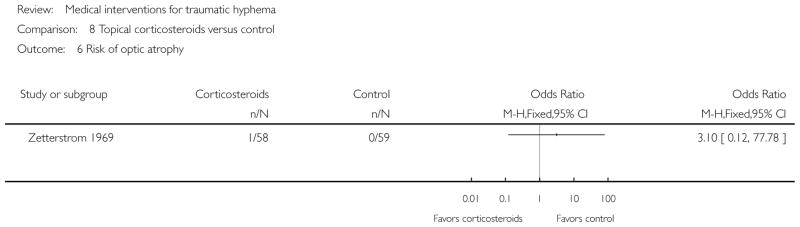
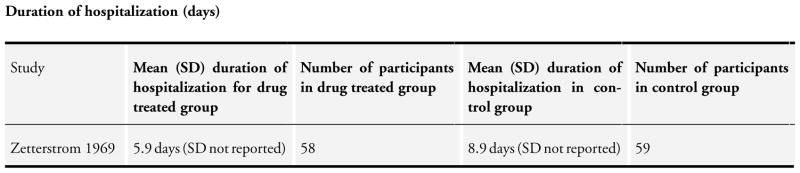
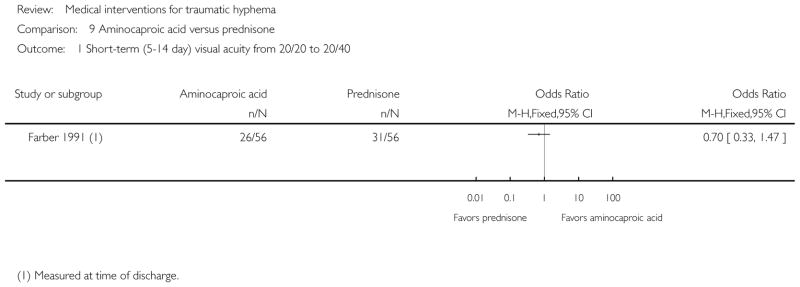
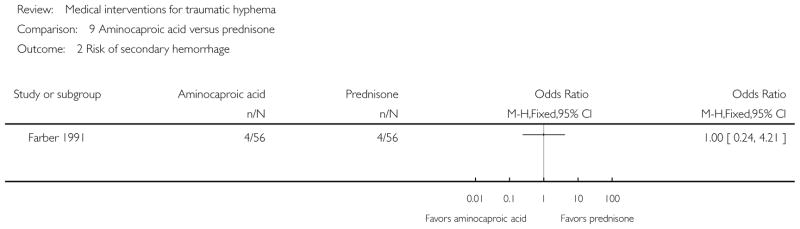
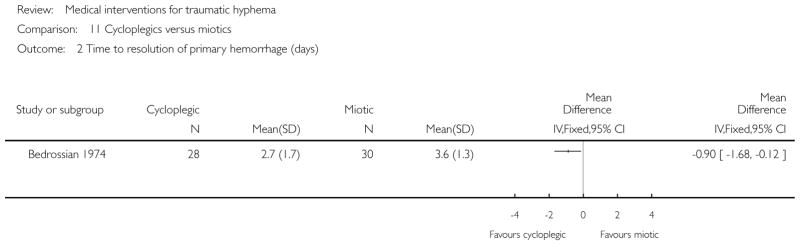
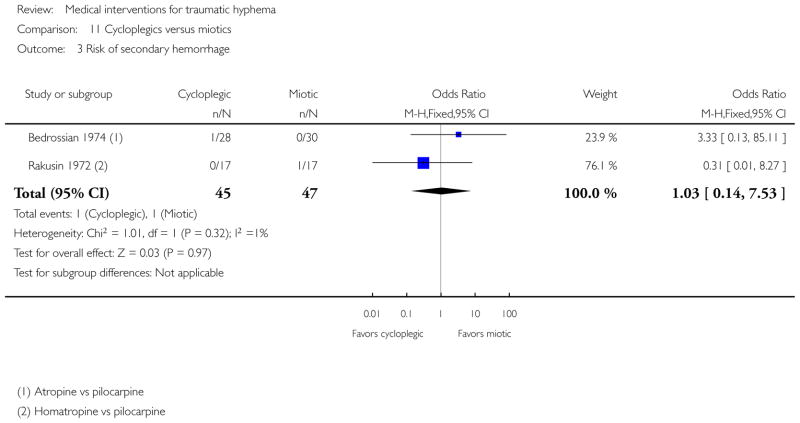
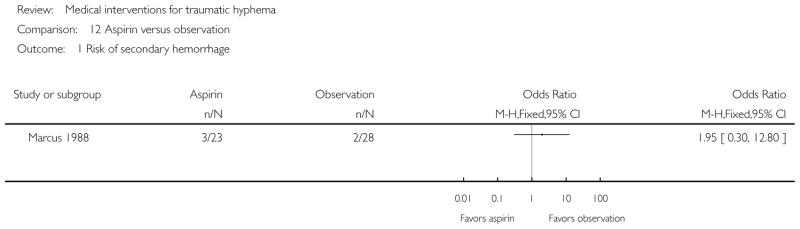
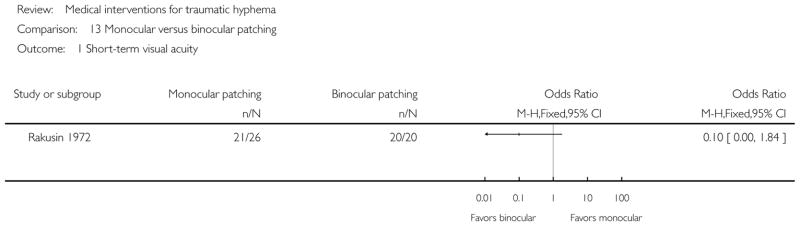
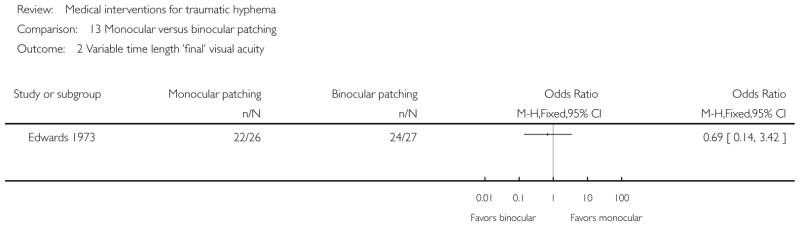
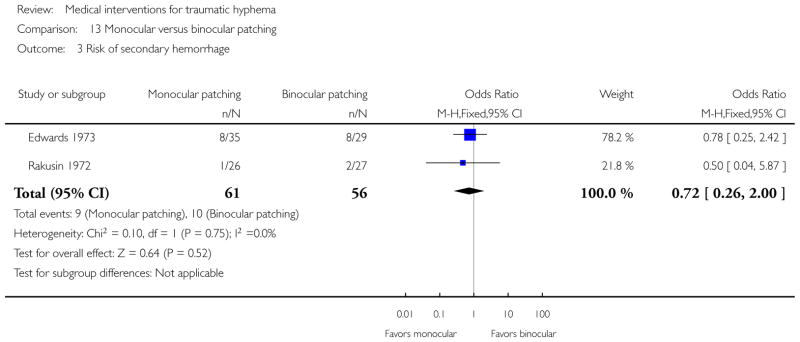
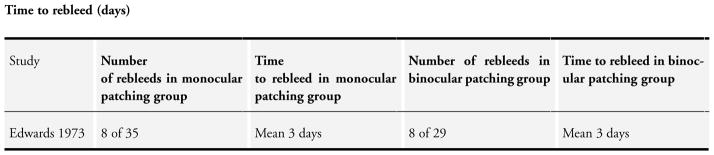
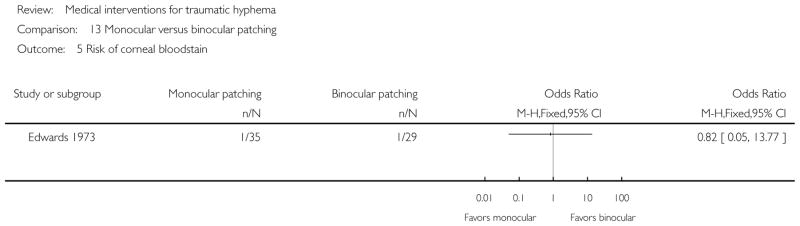
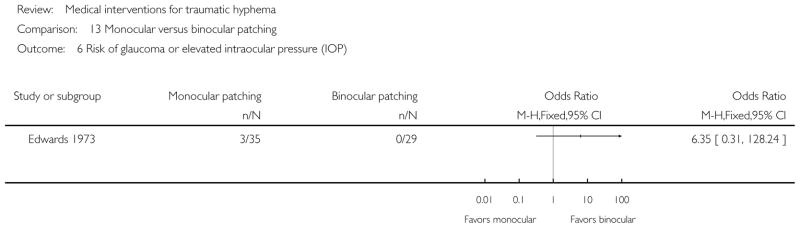
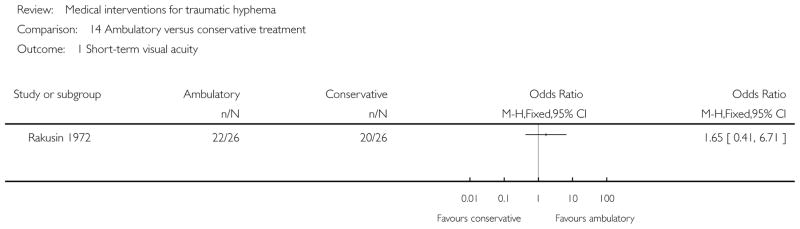
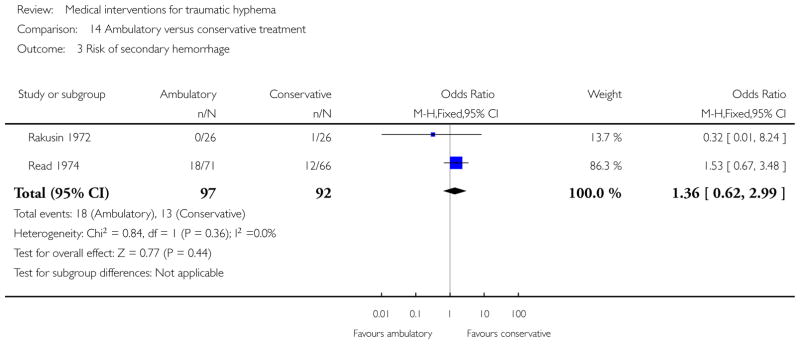
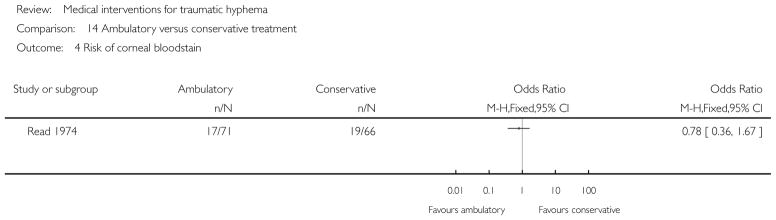
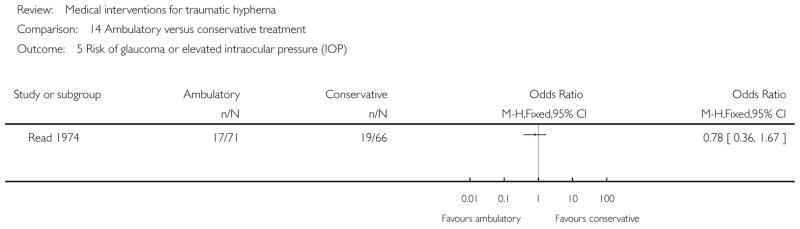
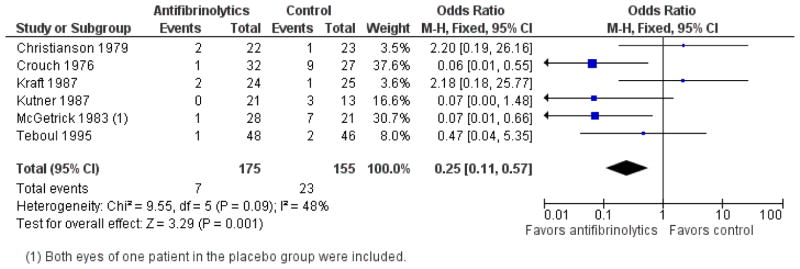
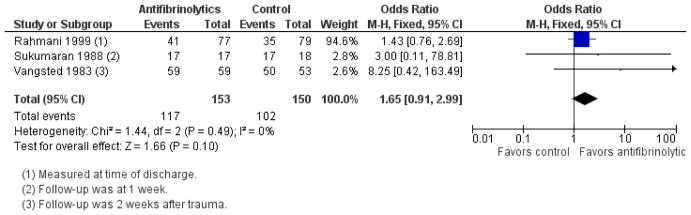
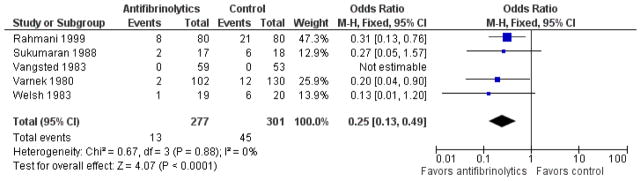
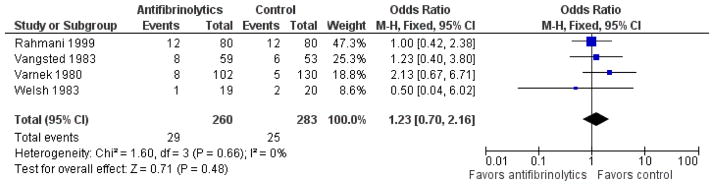
Main results: We included 20 randomized and seven quasi-randomized studies with 2643 participants in this review. Interventions included antifibrinolytic agents (oral and systemic aminocaproic acid, tranexamic acid, and aminomethylbenzoic acid), corticosteroids (systemic and topical), cycloplegics, miotics, aspirin, conjugated estrogens, traditional Chinese medicine, monocular versus bilateral patching, elevation of the head, and bed rest. No intervention had a significant effect on visual acuity whether measured at two weeks or less after the trauma or at longer time periods. The number of days for the primary hyphema to resolve appeared to be longer with the use of aminocaproic acid compared with no use, but was not altered by any other intervention.Systemic aminocaproic acid reduced the rate of recurrent hemorrhage (odds ratio (OR) 0.25, 95% confidence interval (CI) 0.11 to 0.57), but a sensitivity analysis omitting studies not using an intention-to-treat (ITT) analysis reduced the strength of the evidence (OR 0.41, 95% CI 0.16 to 1.09). We obtained similar results for topical aminocaproic acid (OR 0.42, 95% CI 0.16 to 1.10). We found tranexamic acid had a significant effect in reducing the rate of secondary hemorrhage (OR 0.25, 95% CI 0.13 to 0.49), as did aminomethylbenzoic acid as reported in one study (OR 0.07, 95% CI 0.01 to 0.32). The evidence to support an associated reduction in the risk of complications from secondary hemorrhage (i.e. corneal bloodstaining, peripheral anterior synechiae, elevated intraocular pressure, and development of optic atrophy) by antifibrinolytics was limited by the small number of these events. Use of aminocaproic acid was associated with increased nausea, vomiting, and other adverse events compared with placebo. We found no difference in the number of adverse events with the use of systemic versus topical aminocaproic acid or with standard versus lower drug dose. The available evidence on usage of corticosteroids, cycloplegics, or aspirin in traumatic hyphema was limited due to the small numbers of participants and events in the trials.We found no difference in effect between a single versus binocular patch or ambulation versus complete bed rest on the risk of secondary hemorrhage or time to rebleed.
Authors' conclusions: Traumatic hyphema in the absence of other intraocular injuries uncommonly leads to permanent loss of vision. Complications resulting from secondary hemorrhage could lead to permanent impairment of vision, especially in patients with sickle cell trait/disease. We found no evidence to show an effect on visual acuity by any of the interventions evaluated in this review. Although evidence was limited, it appears that patients with traumatic hyphema who receive aminocaproic acid or tranexamic acid are less likely to experience secondary hemorrhaging. However, hyphema in patients treated with aminocaproic acid take longer to clear.Other than the possible benefits of antifibrinolytic usage to reduce the rate of secondary hemorrhage, the decision to use corticosteroids, cycloplegics, or nondrug interventions (such as binocular patching, bed rest, or head elevation) should remain individualized because no solid scientific evidence supports a benefit. As these multiple interventions are rarely used in isolation, further research to assess the additive effect of these interventions might be of value.
Conflict of interest statement
A-MG, HS, RS, and KL: none known.
MG was an investigator for some of the trials included in this review, is a paid consultant for Panoptic Inc (not related to hyphema), and a non-paid board member for Eyetech Inc (not related to hyphema).
Figures




Update of
-
Medical interventions for traumatic hyphema.Cochrane Database Syst Rev. 2011 Jan 19;(1):CD005431. doi: 10.1002/14651858.CD005431.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2013 Dec 03;(12):CD005431. doi: 10.1002/14651858.CD005431.pub3. PMID: 21249670 Free PMC article. Updated.
References
References to studies included in this review
-
- Bedrossian RH. The management of traumatic hyphema. Annals of Ophthalmology. 1974;6(10):1016–8. - PubMed
-
- Christianson MD, Crawford JS. Epsilon aminocaproic acid in the treatment of traumatic hyphema. American Journal of Ophthalmology. 1979;88(4):782.
-
- Crouch ER, Jr, Frenkel M. Aminocaproic acid in the treatment of traumatic hyphema. American Journal of Ophthalmology. 1976;81(3):355–60. - PubMed
-
- Crouch ER, Jr, Williams PB, Gray MK, Crouch ER, Chames M. Topical aminocaproic acid in the treatment of traumatic hyphema. Archives of Ophthalmology. 1997;115(9):1106–12. - PubMed
- Crouch ER, Williams PB. Topical aminocaproic acid in the treatment of patients with traumatic hyphema - reply. Archives of Ophthalmology. 1998;116(3):395–6. - PubMed
-
- Edwards WC, Layden WE. Monocular versus binocular patching in traumatic hyphema. American Journal of Ophthalmology. 1973;76(3):359–62. - PubMed
References to studies excluded from this review
-
- Amirova EKh, Dubilei OV. Experience in the use of streptodecase in the treatment of intraocular hemorrhage. Vestnik Oftalmologii. 1991;107(6):34–6. - PubMed
-
- Anderson TW. Treatment of hyphema with atropinization of contralateral eye. Eye, Ear, Nose & Throat Monthly. 1971;50(7):266–7. - PubMed
-
- Berrios RR, Dreyer EB. Traumatic hyphema. International Ophthalmology Clinics. 1995;35(1):93–103. - PubMed
-
- Bramsen T. Traumatic eye hemorrhage (hyphema) treated with the antifibrinolytic preparation tranexamic acid. Ugeskrift for Laeger. 1977;139(24):1422–4. - PubMed
-
- Bramsen T. The influence of antifibrinolytica on traumatic hyphaema and corneal oedema. Acta Ophthalmologica -Supplementum. 1980;(145):1–53. - PubMed
Additional references
-
- Crouch ER, Jr, Williams PB. Trauma: Ruptures and Bleeding. In: Tasman W, Jaeger EM, editors. Duane’s Clinical Ophthalmology. Vol. 4. Philadelphia, PA: JB Lippincott; 1993. pp. 1–18.
-
- Crouch ER, Jr, Crouch ER. Management of traumatic hyphema: therapeutic options. Journal of Pediatric Ophthalmology and Strabismus. 1999;36(5):238. - PubMed
-
- Deeks JJ, Higgins JPT, Altman DG, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration; 2011. Chapter 9: Analysing data and undertaking meta-analyses. (updated March 2011) Available from www.cochrane-handbook.org.
-
- Goldberg MF. Sickled erythrocytes, hyphema, and secondary glaucoma: I. The diagnosis and treatment of sickled erythrocytes in human hyphemas. Ophthalmic Surgery. 1979;10(4):17–31. - PubMed
-
- Goldberg MF, Dizon R, Moses VK. Sickled erythrocytes, hyphema, and secondary glaucoma: VI. The relationship between intracameral blood cells and aqueous humor pH, PO2, and PCO2. Ophthalmic Surgery. 1979;10(4):78–88. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials