

Prescriptive patient extracorporeal circuit and oxygenator sizing reduces hemodilution and allogeneic blood product transfusion during adult cardiac surgery
- PMID: 24303598
- PMCID: PMC4557535
Prescriptive patient extracorporeal circuit and oxygenator sizing reduces hemodilution and allogeneic blood product transfusion during adult cardiac surgery
Erratum in
- J Extra Corpor Technol. 2014 Mar;46(1):105
Abstract
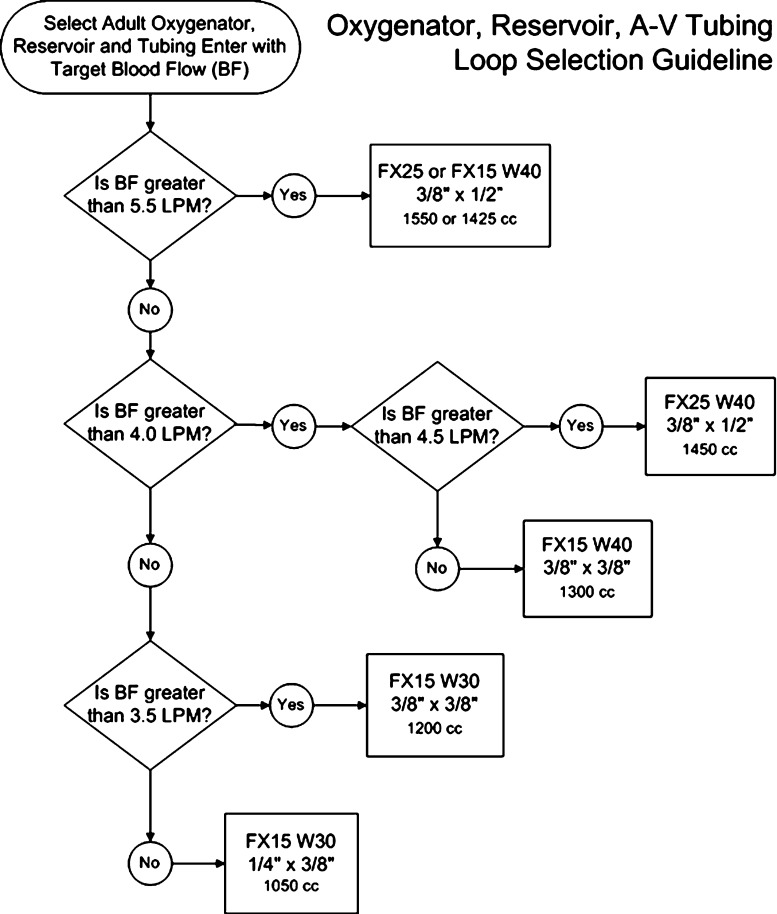
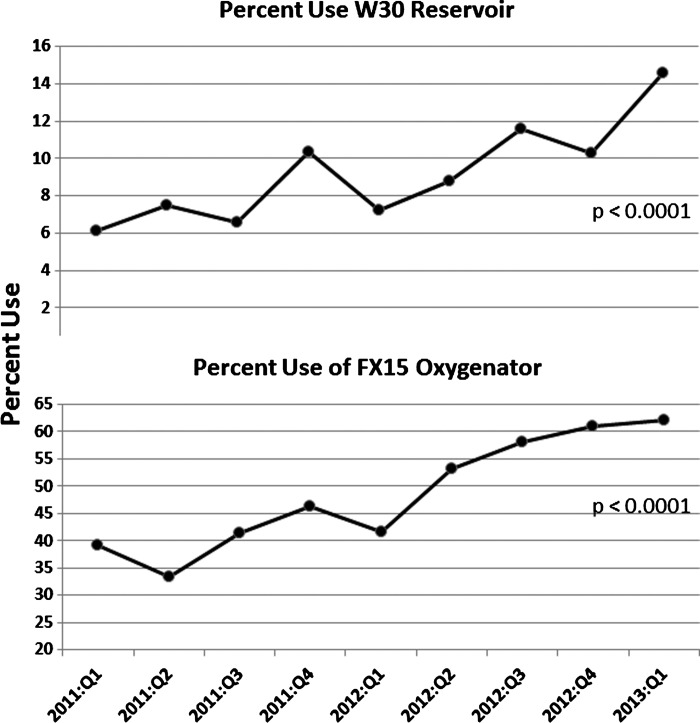
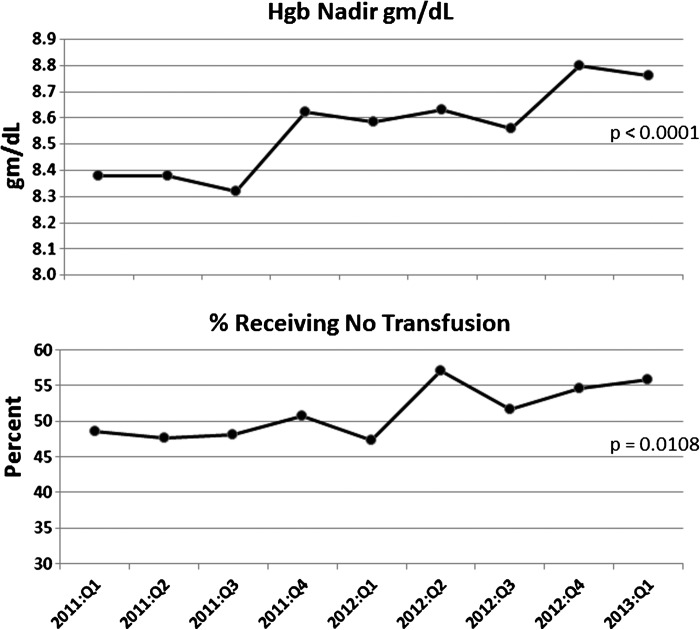
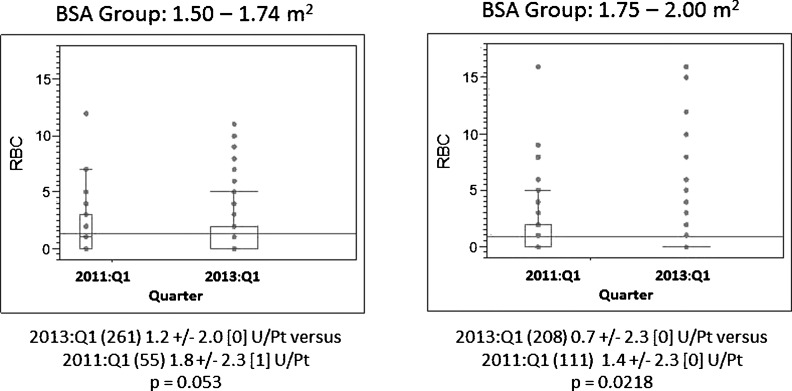
The goal of this cardiopulmonary bypass (CPB) quality improvement initiative was to maximize hemoglobin nadir concentration by minimizing hemodilution and, in turn, eliminating allogeneic blood product transfusion. The effects of transitioning from "one-size-fits-all" to "right-sized" oxygenators, reservoirs, and arterial-venous tubing loops were evaluated through a 2-year retrospective review of 3852 patient perfusion records. Using a sizing algorithm, derived from manufacturers' recommendations, we were able to create individualized "right-sized" extracorporeal circuits based on patient body surface area, cardiac index, and target blood flows. Use of this algorithm led to an increase in the percent of algorithm-recommended smaller oxygenators being used from 39% to 63% (p < .01) and an increase in average hemoglobin nadir from 8.38 to 8.76 g/dL (p < .01). Decreased priming volumes led to increased hemoglobin nadir and decreases in allogeneic blood transfusion (p = .048). Patients with similar body surface areas who previously were exposed to larger oxygenators, reservoirs, and arterial-venous loops were now supported with smaller circuits as a result of the use of the right-sized algorithm. Adjustments to the algorithm were made for unique patients and procedural situations including age, gender, and length and type of procedure. Larger heat exchanger surface area oxygenators were used for circulatory arrest procedures as a result of the need for increased heat exchange capability. Despite the generally higher costs of smaller circuits, reduced transfusion-related expenditures and decreased exposure risks justify the use of smaller circuit components. This quality improvement initiative demonstrated that as an integral part of a multidisciplinary, multimodal blood conservation effort, the use of the "right-sized" circuit algorithm can help to elevate hemoglobin nadir during CPB and eliminate allogeneic blood transfusions to patients undergoing CPB.
Keywords: cardiopulmonary bypass, oxygenator, perfusion index, extracorporeal circuit, hemodilution.
Conflict of interest statement
Jeffrey B. Riley has received honoraria for scientific presentations by Sorin USA and Terumo, in the past.
Figures
Comment in
-
Going beyond manufacturers' limitations is not in the best interest of our patients.J Extra Corpor Technol. 2014 Mar;46(1):101-2. J Extra Corpor Technol. 2014. PMID: 24779128 Free PMC article. No abstract available.
-
Response to letter "Going beyond manufacturers' limitations is not in the best interests of our patients" by Gerard J. Myers.J Extra Corpor Technol. 2014 Mar;46(1):103-4. J Extra Corpor Technol. 2014. PMID: 24779129 No abstract available.
References
-
- Ranucci M, Pazzaglia A, Bianchini C, Bozzetti G, Isgro G.. Body size, gender, and transfusions as determinants of outcome after coronary operations. Ann Thorac Surg. 2008;85:481–486. - PubMed
-
- Loor G, Li L, Sabik JF 3rd, Rajeswaran J, Blackstone EH, Koch CG.. Nadir hematocrit during cardiopulmonary bypass: End-organ dysfunction and mortality. J Thorac Cardiovasc Surg. 2012;144:654–662. - PubMed
-
- DeFoe GR, Ross CS, Olmstead EM, et al. Lowest hematocrit on bypass and adverse outcomes associated with coronary artery bypass grafting. Northern New England Cardiovascular Disease Study Group. Ann Thorac Surg. 2001;71:769–776. - PubMed
-
- Fang WC, Helm RE, Krieger KH, et al. Impact of minimum hematocrit during cardiopulmonary bypass on mortality in patients undergoing coronary artery surgery. Circulation. 1997;96:II-194–II-199. - PubMed
-
- Karkouti K, O’Farrell R, Yau TM, Beattie WS.. Prediction of massive blood transfusion in cardiac surgery. Can J Anaesth. 2006;53:781–794. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources