

Changes in geometric configuration and biomechanical parameters of a rapidly growing abdominal aortic aneurysm may provide insight in aneurysms natural history and rupture risk
- PMID: 24304476
- PMCID: PMC4235172
- DOI: 10.1186/1742-4682-10-67
Changes in geometric configuration and biomechanical parameters of a rapidly growing abdominal aortic aneurysm may provide insight in aneurysms natural history and rupture risk
Abstract
Background: Abdominal aortic aneurysms (AAA) are currently being treated based on the maximum diameter criterion which has often been proven insufficient to determine rupture risk in case of every AAA. We analyzed a rare case of an AAA which presented an extremely fast growth focusing on biomechanical determinants that may indicate a high risk profile. The examination of such a case is expected to motivate future research towards patient-specific rupture risk estimations.
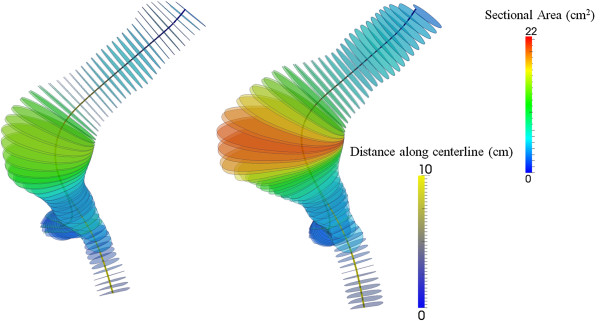
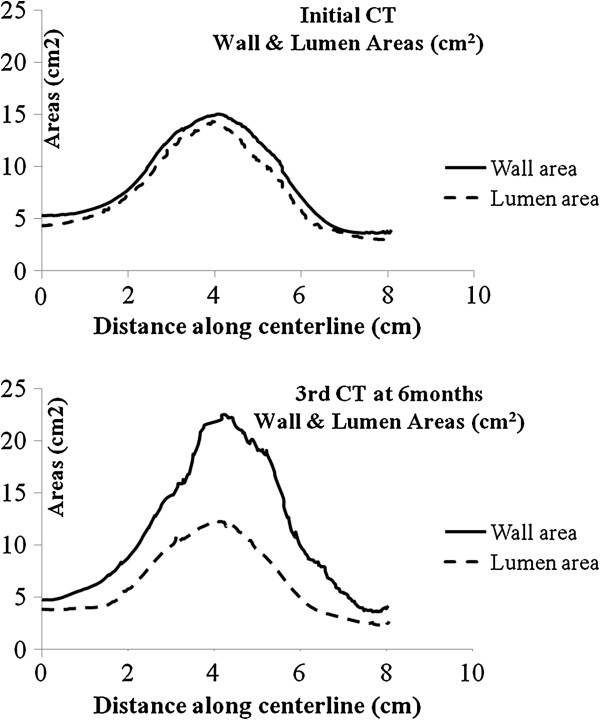
Methods: An initially small AAA (maximum diameter: 4.5 cm) was followed-up and presented a growth of 1 cm in only 6-months of surveillance becoming suitable for surgical repair. Changes of morphometric characteristics regarding AAA, thrombus and lumen volumes, cross-sectional areas, thrombus maximum thickness and eccentricity, and maximum centerline curvature were recorded. Moreover biomechanical variables concerning Peak Wall Stress, AAA surface area exposed to high stress and redistribution of stress during follow-up were also assessed.
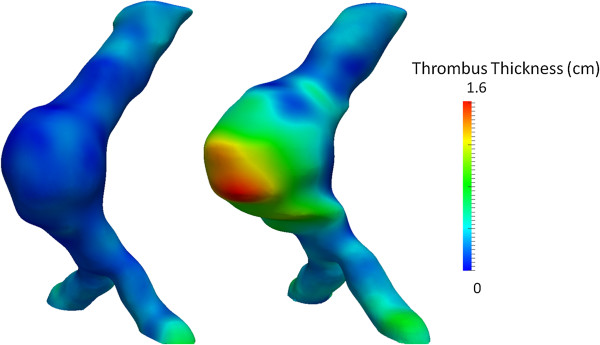
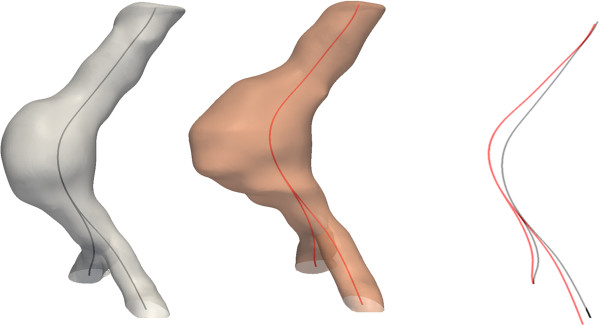
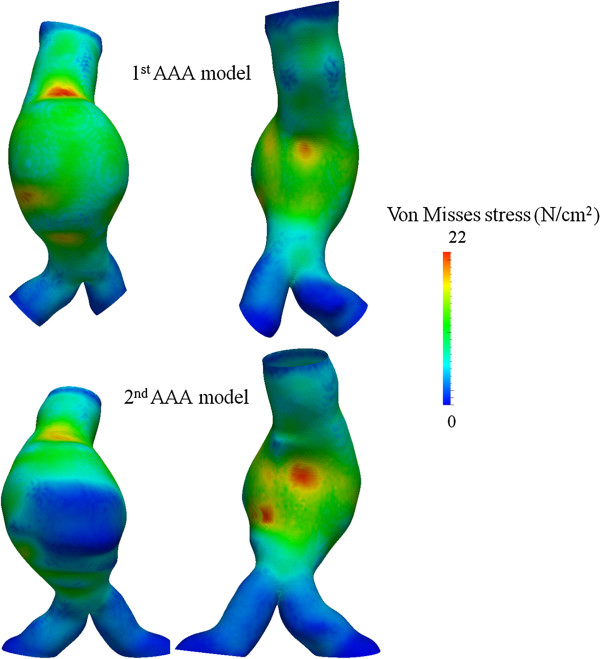
Results: Total aneurysm volume increased from 85 to 120 ml which regarded thrombus deposition since lumen volume remained stable. Thrombus deposition was eccentric regarding anterior AAA segment while its thickness increased from 0.3 cm to 1.6 cm. Moreover there was an anterior bulging over time as depicted by an increase in maximum centerline curvature from 0.4 cm-1 to 0.5 cm-1. Peak Wall Stress (PWS) exerted on aneurysm wall did not change significantly over time, slightly decreasing from 22 N/cm2 to 21 N/cm2. At the same time the area under high wall stress remained practically constant (9.9 cm2 at initial vs 9.7 cm2 at final examination) but there was a marked redistribution of wall stress against the posterior aneurysmal wall over time.
Conclusion: Aneurysm area under high stress and redistribution of stress against the posterior wall due to changes in geometric configuration and thrombus deposition over time may have implications to aneurysms natural history and rupture risk.
Figures
References
-
- Minino AM, Heron MP, Murphy SL, Kochanek KD. Deaths: final data for 2004. National Vital Stat Rep. 2007;55:1–119. - PubMed
-
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005. Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113:463–654. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
