

A global survey of changing patterns of food allergy burden in children
- PMID: 24304599
- PMCID: PMC3879010
- DOI: 10.1186/1939-4551-6-21
A global survey of changing patterns of food allergy burden in children
Abstract
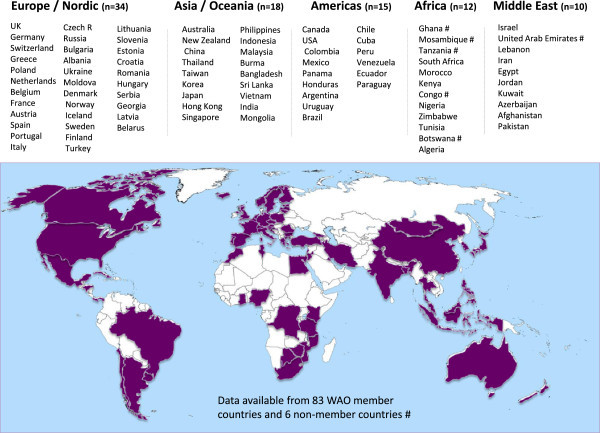
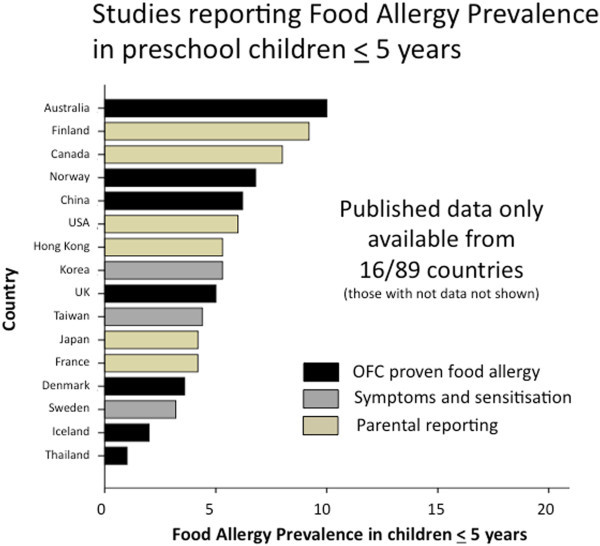
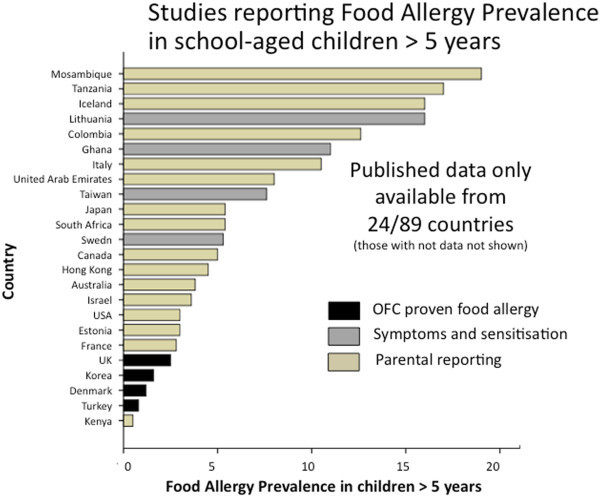
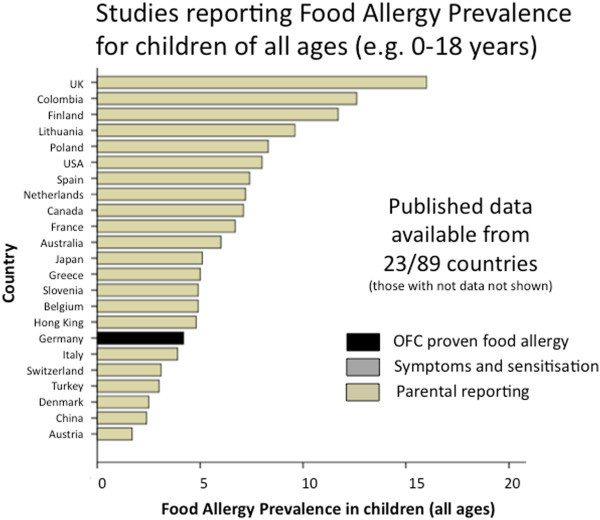
While food allergies and eczema are among the most common chronic non-communicable diseases in children in many countries worldwide, quality data on the burden of these diseases is lacking, particularly in developing countries. This 2012 survey was performed to collect information on existing data on the global patterns and prevalence of food allergy by surveying all the national member societies of the World Allergy Organization, and some of their neighbouring countries. Data were collected from 89 countries, including published data, and changes in the health care burden of food allergy. More than half of the countries surveyed (52/89) did not have any data on food allergy prevalence. Only 10% (9/89) of countries had accurate food allergy prevalence data, based on oral food challenges (OFC). The remaining countries (23/89) had data largely based on parent-reporting of a food allergy diagnosis or symptoms, which is recognised to overestimate the prevalence of food allergy. Based on more accurate measures, the prevalence of clinical (OFC proven) food allergy in preschool children in developed countries is now as high as 10%. In large and rapidly emerging societies of Asia, such as China, where there are documented increases in food allergy, the prevalence of OFC-proven food allergy is now around 7% in pre-schoolers, comparable to the reported prevalence in European regions. While food allergy appears to be increasing in both developed and developing countries in the last 10-15 years, there is a lack of quality comparative data. This survey also highlights inequities in paediatric allergy services, availability of adrenaline auto-injectors and standardised National Anaphylaxis Action plans. In conclusion, there remains a need to gather more accurate data on the prevalence of food allergy in many developed and developing countries to better anticipate and address the rising community and health service burden of food allergy.
Figures
References
-
- Osborne NJ, Koplin JJ, Martin PE, Gurrin LC, Lowe AJ, Matheson MC. et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J Allergy Clin Immunol. 2011;6:668–676. doi: 10.1016/j.jaci.2011.01.039. e1-2. - DOI - PubMed
-
- Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK. et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;6:733–743. doi: 10.1016/S0140-6736(06)69283-0. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
