

Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades
- PMID: 24305718
- PMCID: PMC3922507
- DOI: 10.1093/neuonc/not158
Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades
Abstract
Background: Amide proton transfer (APT) imaging is a novel molecular MRI technique to detect endogenous mobile proteins and peptides through chemical exchange saturation transfer. We prospectively assessed the usefulness of APT imaging in predicting the histological grade of adult diffuse gliomas.
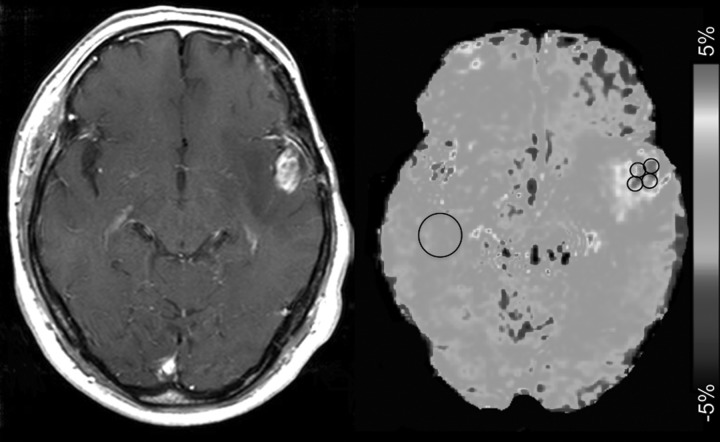
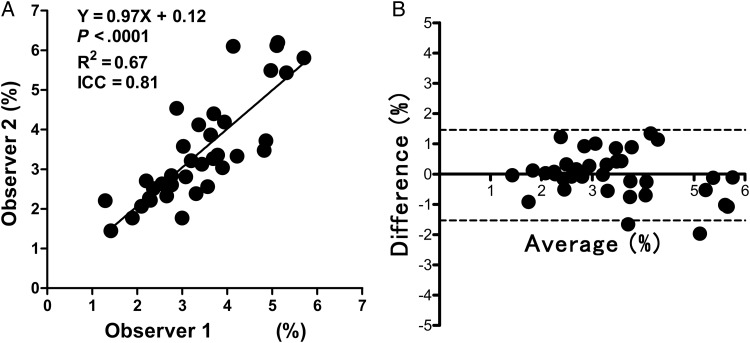
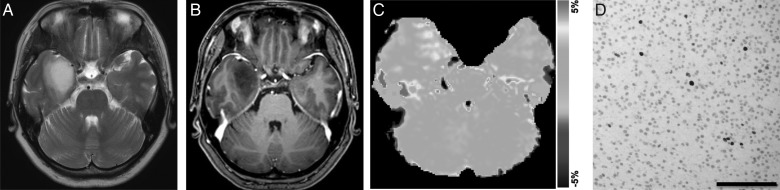
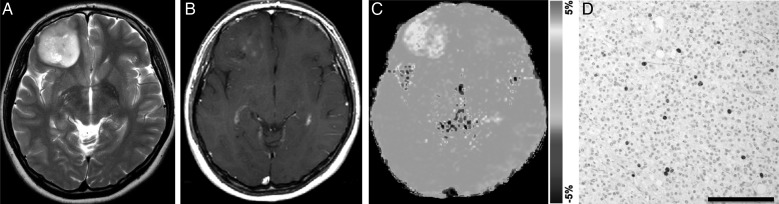
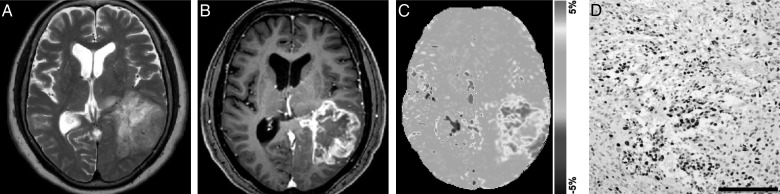
Methods: Thirty-six consecutive patients with histopathologically proven diffuse glioma (48.1 ± 14.7 y old, 16 males and 20 females) were included in the study. APT MRI was conducted on a 3T clinical scanner and was obtained with 2 s saturation at 25 saturation frequency offsets ω = -6 to +6 ppm (step 0.5 ppm). δB0 maps were acquired separately for a point-by-point δB0 correction. APT signal intensity (SI) was defined as magnetization transfer asymmetry at 3.5 ppm: magnetization transfer ratio (MTR)asym = (S[-3.5 ppm] - S[+3.5 ppm])/S0. Regions of interest were carefully placed by 2 neuroradiologists in solid parts within brain tumors. The APT SI was compared with World Health Organization grade, Ki-67 labeling index (LI), and cell density.
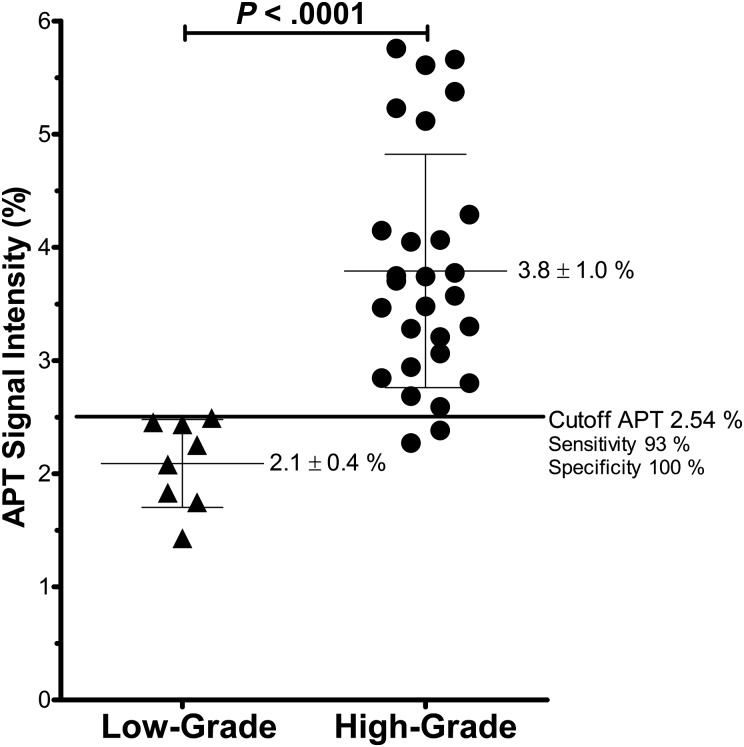
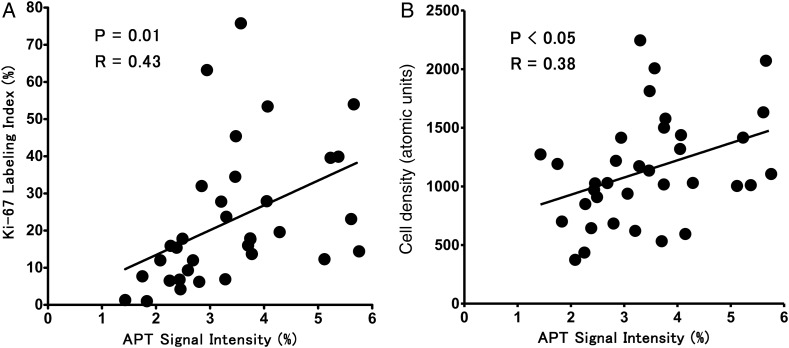
Results: The mean APT SI values were 2.1 ± 0.4% in grade II gliomas (n = 8), 3.2 ± 0.9% in grade III gliomas (n = 10), and 4.1 ± 1.0% in grade IV gliomas (n = 18). Significant differences in APT intensity were observed between grades II and III (P < .05) and grades III and IV (P < .05), as well as between grades II and IV (P < .001). There were positive correlations between APT SI and Ki-67 LI (P = .01, R = 0.43) and between APT SI and cell density (P < .05, R = 0.38). The gliomas with microscopic necrosis showed higher APT SI than those without necrosis (P < .001).
Conclusions: APT imaging can predict the histopathological grades of adult diffuse gliomas.
Keywords: amide proton transfer (APT) imaging; chemical exchange saturation transfer (CEST); glioma..
Figures
References
-
- Clarke J, Butowski N, Chang S. Recent advances in therapy for glioblastoma. Arch Neurol. 2010;67(3):279–283. - PubMed
-
- Dean BL, Drayer BP, Bird CR, et al. Gliomas: classification with MR imaging. Radiology. 1990;174(2):411–415. - PubMed
-
- Felix R, Schorner W, Laniado M, et al. Brain tumors: MR imaging with gadolinium-DTPA. Radiology. 1985;156(3):681–688. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
