

The prevalence of low serum vitamin B-12 status in the absence of anemia or macrocytosis did not increase among older U.S. adults after mandatory folic acid fortification
- PMID: 24306216
- PMCID: PMC5291239
- DOI: 10.3945/jn.113.183095
The prevalence of low serum vitamin B-12 status in the absence of anemia or macrocytosis did not increase among older U.S. adults after mandatory folic acid fortification
Abstract
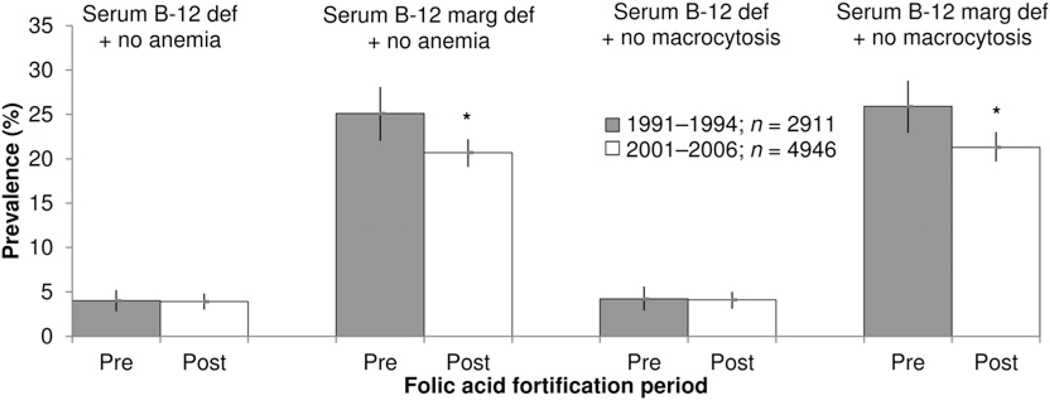
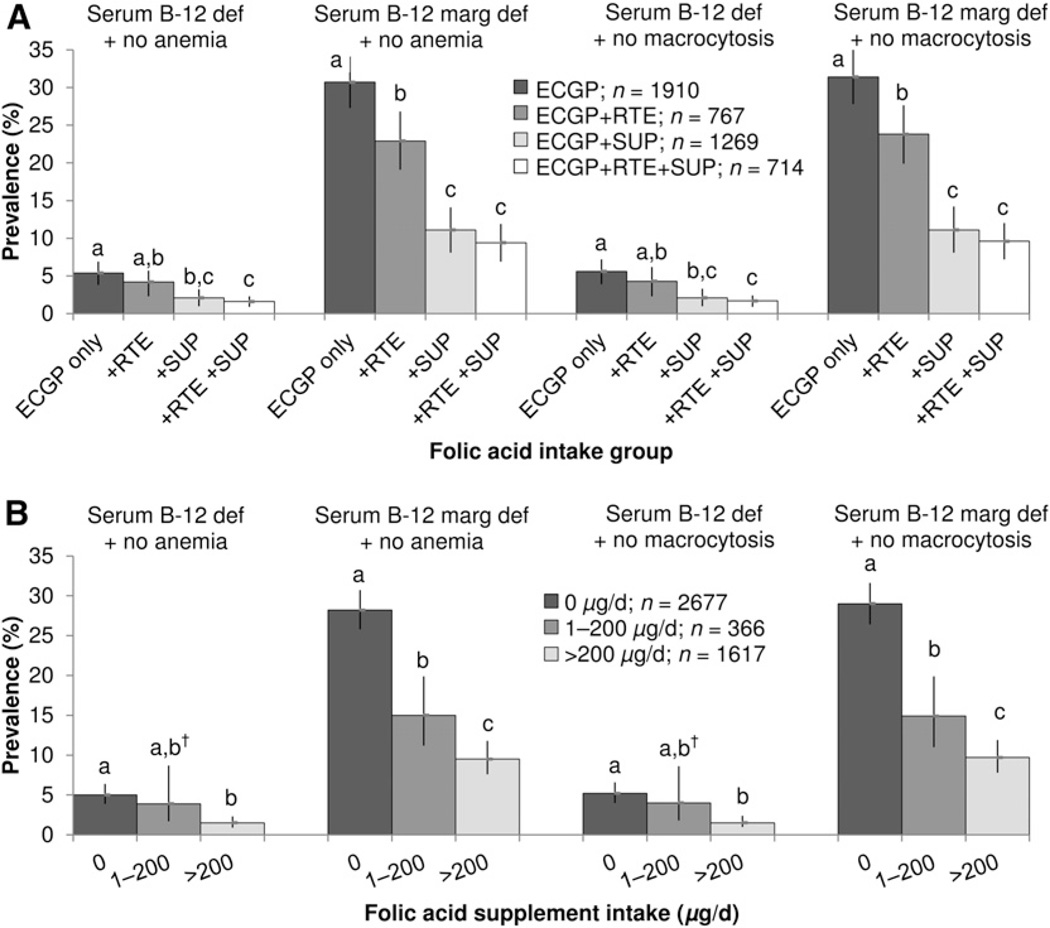
Whether folic acid fortification and supplementation at the population level have led to a higher prevalence of vitamin B-12 deficiency in the absence of anemia remains to be examined among a nationally representative sample of older U.S. adults. We assessed the prevalence of low vitamin B-12 status in the absence of anemia or macrocytosis before and after fortification among adults aged >50 y using cross-sectional data from the NHANES 1991-1994 (prefortification) and 2001-2006 (postfortification). We compared the prefortification and postfortification prevalence of multiple outcomes, including serum vitamin B-12 deficiency (<148 pmol/L) and marginal deficiency (148-258 pmol/L) with and without anemia (hemoglobin <130 g/L for men, <120 g/L for women) and with and without macrocytosis (mean cell volume >100 fL) using multinomial logistic regression, adjusting for age, sex, ethnicity, body mass index, C-reactive protein, and vitamin B-12 supplement use. Prefortification and postfortification serum vitamin B-12 deficiency without anemia [4.0 vs. 3.9%; adjusted prevalence ratio (aPR) (95% CI): 0.98 (0.67, 1.44)] or without macrocytosis [4.2 vs. 4.1%; aPR (95% CI): 0.96 (0.65, 1.43)] remained unchanged. Marginal deficiency without anemia [25.1 vs. 20.7%; aPR (95% CI): 0.82 (0.72, 0.95)] or without macrocytosis [25.9 vs. 21.3%; aPR (95% CI): 0.82 (0.72, 0.94)] were both significantly lower after fortification. After fortification, higher folic acid intake was associated with a lower prevalence of low serum B-12 status in the absence of anemia or macrocytosis. Results suggest that the prevalence of low serum B-12 status in the absence of anemia or macrocytosis among older U.S. adults did not increase after fortification. Thus, at the population level, we found no evidence to support concerns that folic acid adversely affected the clinical presentation of vitamin B-12 deficiency among older adults.
Conflict of interest statement
2 Author disclosures: Y. P. Qi, A. N. Do, H. C. Hamner, C. M. Pfeiffer, and R. J. Berry, no conflicts of interest.
Figures
References
-
- Chanarin I. Historical review: a history of pernicious anaemia. Br J Haematol. 2000;111:407–415. - PubMed
-
- Hoffbrand AV, Weir DG. The history of folic acid. Br J Haematol. 2001;113:579–589. - PubMed
-
- Savage DG, Linedenbaum J. Folate-coblamin interactions. In: Bailey LB, editor. Folate in health and disease. New York: Marcel Dekker; 1995. pp. 237–285.
-
- Vilter CF, Vilter RW, Spies TD. The treatment of pernicious and related anemias with synthetic folic acid; observations on the maintenance of a normal hematologic status and on the occurrence of combined system disease at the end of one year. J Lab Clin Med. 1947;32:262–273. - PubMed
-
- Ross JF, Belding H, Paegel BL. The development and progression of subacute combined degeneration of the spinal cord in patients with pernicious anemia treated with synthetic pteroylglutamic (folic) acid. Blood. 1948;3:68–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
