

Three-dimensional whole-brain perfusion quantification using pseudo-continuous arterial spin labeling MRI at multiple post-labeling delays: accounting for both arterial transit time and impulse response function
- PMID: 24307572
- PMCID: PMC3947417
- DOI: 10.1002/nbm.3040
Three-dimensional whole-brain perfusion quantification using pseudo-continuous arterial spin labeling MRI at multiple post-labeling delays: accounting for both arterial transit time and impulse response function
Abstract
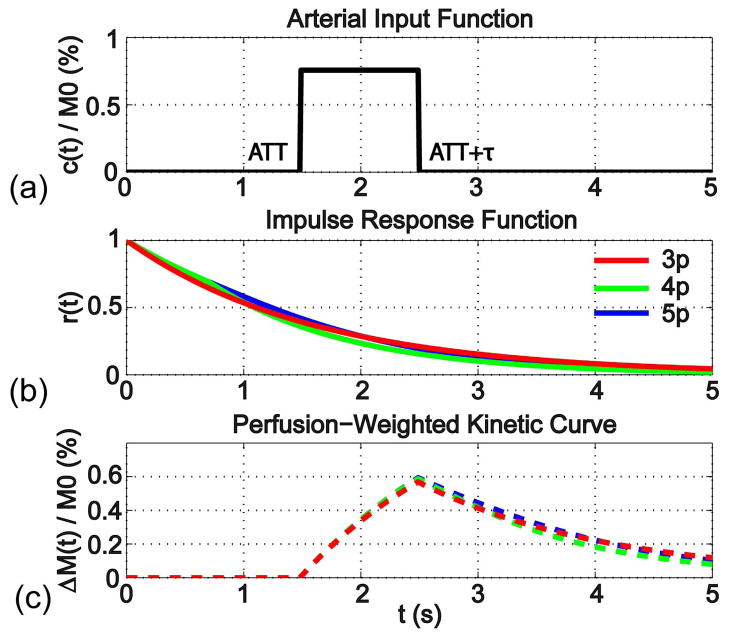
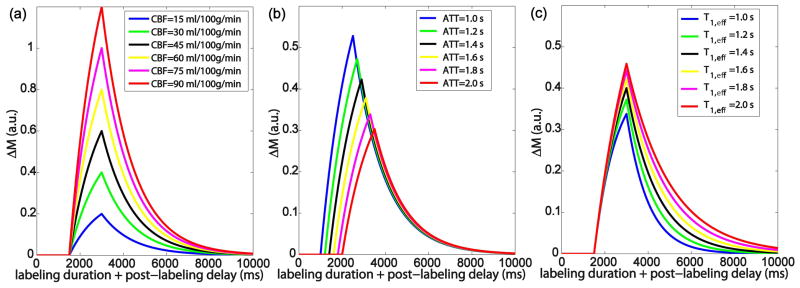
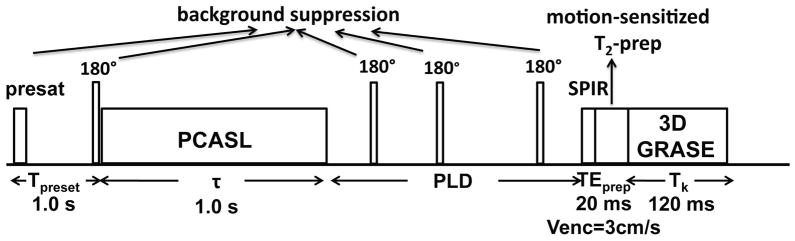
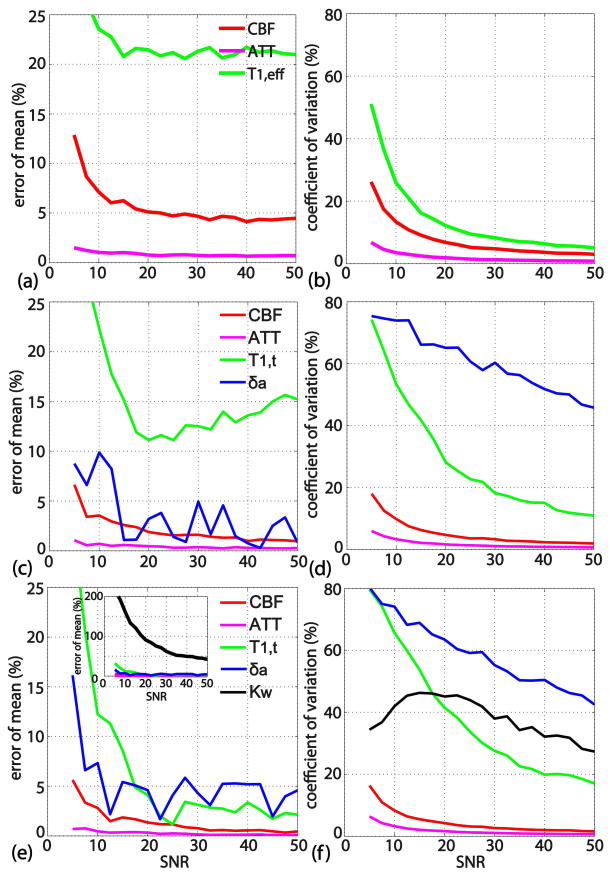
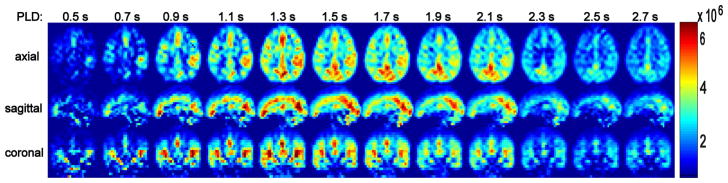
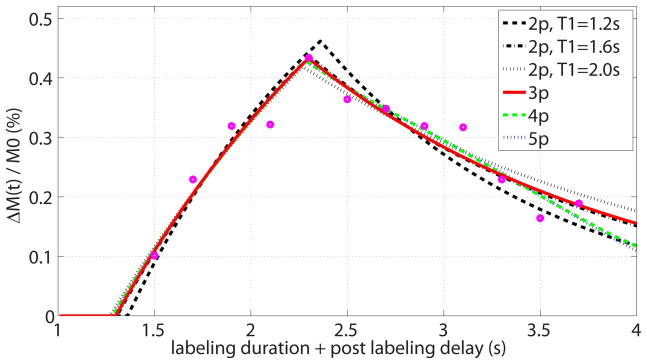
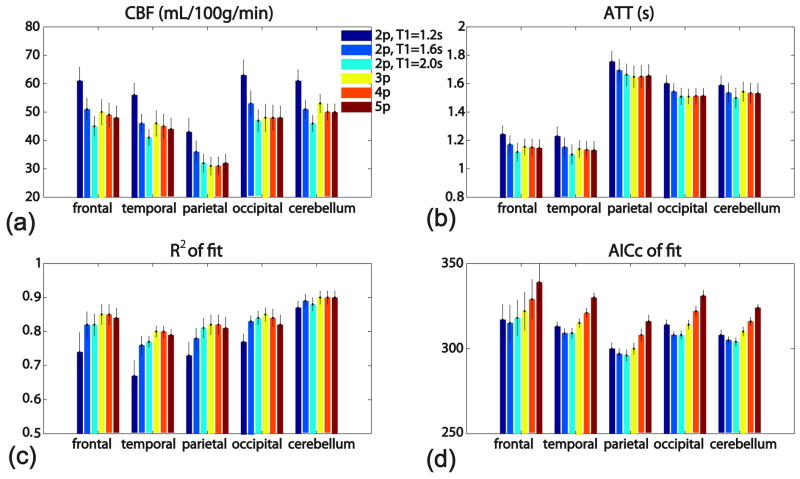
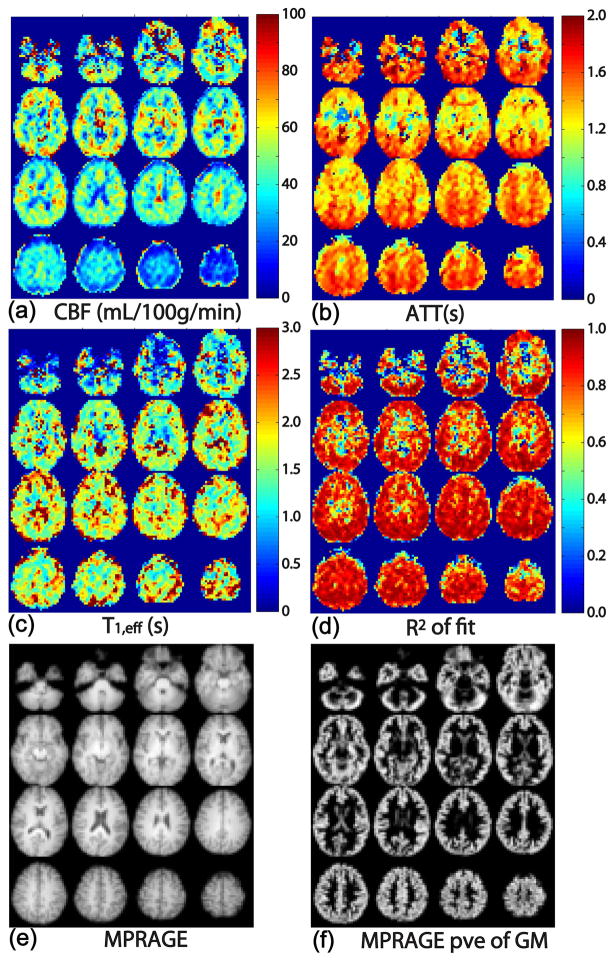
Measurement of the cerebral blood flow (CBF) with whole-brain coverage is challenging in terms of both acquisition and quantitative analysis. In order to fit arterial spin labeling-based perfusion kinetic curves, an empirical three-parameter model which characterizes the effective impulse response function (IRF) is introduced, which allows the determination of CBF, the arterial transit time (ATT) and T(1,eff). The accuracy and precision of the proposed model were compared with those of more complicated models with four or five parameters through Monte Carlo simulations. Pseudo-continuous arterial spin labeling images were acquired on a clinical 3-T scanner in 10 normal volunteers using a three-dimensional multi-shot gradient and spin echo scheme at multiple post-labeling delays to sample the kinetic curves. Voxel-wise fitting was performed using the three-parameter model and other models that contain two, four or five unknown parameters. For the two-parameter model, T(1,eff) values close to tissue and blood were assumed separately. Standard statistical analysis was conducted to compare these fitting models in various brain regions. The fitted results indicated that: (i) the estimated CBF values using the two-parameter model show appreciable dependence on the assumed T(1,eff) values; (ii) the proposed three-parameter model achieves the optimal balance between the goodness of fit and model complexity when compared among the models with explicit IRF fitting; (iii) both the two-parameter model using fixed blood T1 values for T(1,eff) and the three-parameter model provide reasonable fitting results. Using the proposed three-parameter model, the estimated CBF (46 ± 14 mL/100 g/min) and ATT (1.4 ± 0.3 s) values averaged from different brain regions are close to the literature reports; the estimated T(1,eff) values (1.9 ± 0.4 s) are higher than the tissue T1 values, possibly reflecting a contribution from the microvascular arterial blood compartment.
Keywords: GRASE; PCASL; arterial transit time; brain; cerebral blood flow; clinical; human; impulse response function.
Copyright © 2013 John Wiley & Sons, Ltd.
Figures
References
-
- Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998;40(3):383–396. - PubMed
-
- Buxton RB. Quantifying CBF with arterial spin labeling. J Magn Reson Imaging. 2005;22(6):723–726. - PubMed
-
- Alsop DC, Detre JA. Reduced transit-time sensitivity in noninvasive magnetic resonance imaging of human cerebral blood flow. J Cereb Blood Flow Metab. 1996;16(6):1236–1249. - PubMed
-
- Wang J, Alsop DC, Song HK, Maldjian JA, Tang K, Salvucci AE, Detre JA. Arterial transit time imaging with flow encoding arterial spin tagging (FEAST) Magn Reson Med. 2003;50(3):599–607. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
