

Small cell carcinoma of the liver and biliary tract without jaundice
- PMID: 24307811
- PMCID: PMC3848165
- DOI: 10.3748/wjg.v19.i44.8146
Small cell carcinoma of the liver and biliary tract without jaundice
Abstract
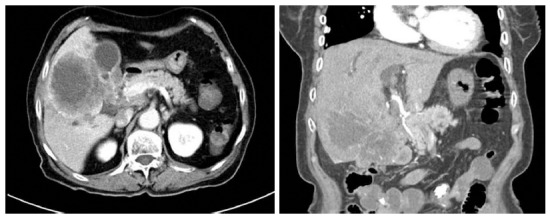
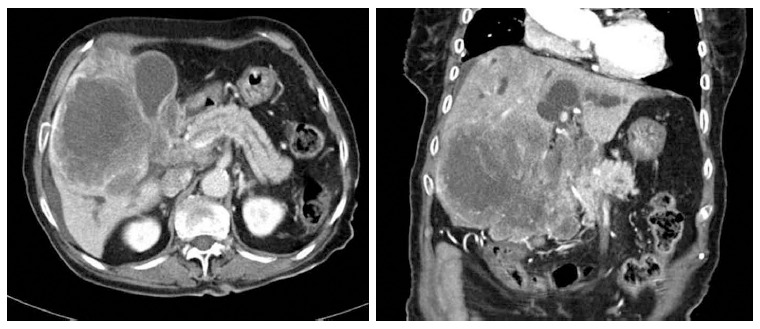
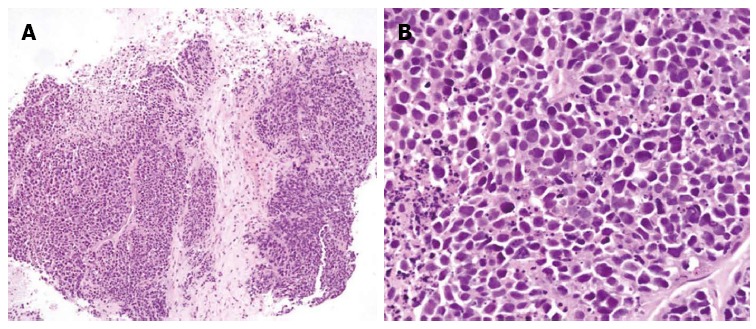
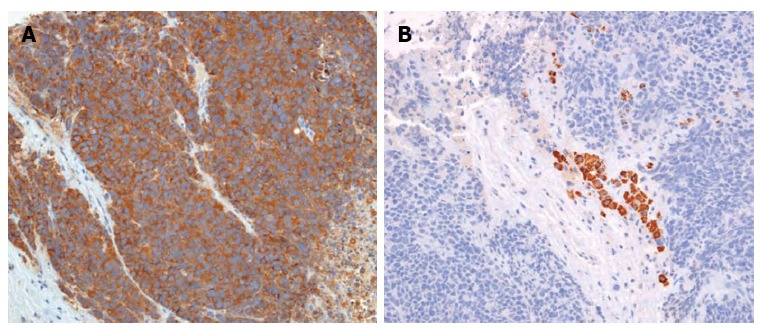
An 80-year-old woman presenting with chest pain was found to have a large, lobulated soft tissue mass in the liver and nearby tissues on abdominal computed tomography (CT). The tumor had invaded the common hepatic artery and main portal vein. Jaundice developed 4 wk later, at which point, a pancreas and biliary CT scan revealed a large mass in the right lobe of the liver and a hilar duct obstruction, which was found to be a small cell carcinoma. Despite its rarity, liver and bile duct small cell carcinoma should be considered in the differential diagnosis of atypical chest pain without jaundice.
Keywords: Bile duct mass; Extrapulmonary small cell carcinoma; Jaundice; Liver mass; Neuroendocrine tumor.
Figures
Similar articles
-
[Diagnostic value of computed tomography for the detection of invasion of the caudate bile duct branch in carcinoma of the hepatic hilum].Nihon Geka Gakkai Zasshi. 1988 Jun;89(6):889-97. Nihon Geka Gakkai Zasshi. 1988. PMID: 2847003 Japanese.
-
Surgical treatment of a patient with diaphragmatic invasion by a ruptured hepatocellular carcinoma with biliary and portal venous tumor thrombi.J Nippon Med Sch. 2012;79(2):147-52. doi: 10.1272/jnms.79.147. J Nippon Med Sch. 2012. PMID: 22687359
-
S4a + S5 with caudate lobe (S1) resection using the Taj Mahal liver parenchymal resection for carcinoma of the biliary tract.J Gastrointest Surg. 1999 Jul-Aug;3(4):369-73. doi: 10.1016/s1091-255x(99)80052-3. J Gastrointest Surg. 1999. PMID: 10482688
-
Hepatocellular carcinoma with obstructive jaundice: diagnosis, treatment and prognosis.World J Gastroenterol. 2003 Mar;9(3):385-91. doi: 10.3748/wjg.v9.i3.385. World J Gastroenterol. 2003. PMID: 12632482 Free PMC article. Review.
-
Intraductal papillary neoplasm of the bile ducts: A case report and literature review.World J Gastroenterol. 2015 Nov 21;21(43):12498-504. doi: 10.3748/wjg.v21.i43.12498. World J Gastroenterol. 2015. PMID: 26604656 Free PMC article. Review.
Cited by
-
Pulmonary Tumor Thrombotic Microangiopathy Suspected to be COVID-19 Vaccine-Related Myocarditis: A Case Report.Cureus. 2024 Mar 24;16(3):e56803. doi: 10.7759/cureus.56803. eCollection 2024 Mar. Cureus. 2024. PMID: 38654790 Free PMC article.
-
Re-Recognizing the Cellular Origin of the Primary Epithelial Tumors of the Liver.J Hepatocell Carcinoma. 2021 Dec 7;8:1537-1563. doi: 10.2147/JHC.S334935. eCollection 2021. J Hepatocell Carcinoma. 2021. PMID: 34917552 Free PMC article. Review.
-
Undifferentiated carcinoma of the liver: a case report with immunohistochemical analysis.Surg Case Rep. 2017 Dec;3(1):12. doi: 10.1186/s40792-017-0288-0. Epub 2017 Jan 10. Surg Case Rep. 2017. PMID: 28074442 Free PMC article.
References
-
- Levenson RM, Ihde DC, Matthews MJ, Cohen MH, Gazdar AF, Bunn PA, Minna JD. Small cell carcinoma presenting as an extrapulmonary neoplasm: sites of origin and response to chemotherapy. J Natl Cancer Inst. 1981;67:607–612. - PubMed
-
- Remick SC, Ruckdeschel JC. Extrapulmonary and pulmonary small-cell carcinoma: tumor biology, therapy, and outcome. Med Pediatr Oncol. 1992;20:89–99. - PubMed
-
- Richardson RL, Weiland LH. Undifferentiated small cell carcinomas in extrapulmonary sites. Semin Oncol. 1982;9:484–496. - PubMed
-
- Ryu SH, Han SY, Suh SH, Koo YH, Cho JH, Han SH, Lee SW, Cho JH, Jeong JS. [A case of primary small cell carcinoma of the liver] Korean J Hepatol. 2005;11:289–292. - PubMed
-
- Kim YH, Kwon R, Jung GJ, Roh MH, Han SY, Kwon HC, Jeong JS, Shin TB, Oh JY, Lee KN. Extrapulmonary small-cell carcinoma of the liver. J Hepatobiliary Pancreat Surg. 2004;11:333–337. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
