

A tailored implementation intervention to implement recommendations addressing polypharmacy in multimorbid patients: study protocol of a cluster randomized controlled trial
- PMID: 24308282
- PMCID: PMC4234123
- DOI: 10.1186/1745-6215-14-420
A tailored implementation intervention to implement recommendations addressing polypharmacy in multimorbid patients: study protocol of a cluster randomized controlled trial
Abstract
Background: Multimorbid patients frequently receive complex medication regimens and are at higher risk for adverse drug reactions and hospitalisations. Managing patients with polypharmacy is demanding, because it requires coordination of multiple prescribers and intensive monitoring. Three evidence-based recommendations addressing polypharmacy in primary care are structured medication counselling, use of medication lists and medication reviews to avoid potentially inappropriate medication (PIM). Although promising to improve patient outcomes, these recommendations are not well implemented in German routine care. Implementation of guidelines is often hindered by specific "determinants of change". "Tailored" interventions are designed to specifically address previously identified determinants. This study examines a tailored intervention to implement the aforementioned recommendations into German primary care practices. This study is part of the European Tailored Interventions for Chronic Diseases project, which aims at contributing knowledge about the methods used for tailoring.
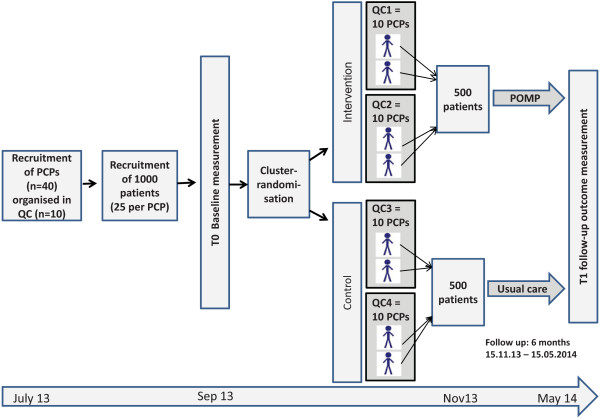
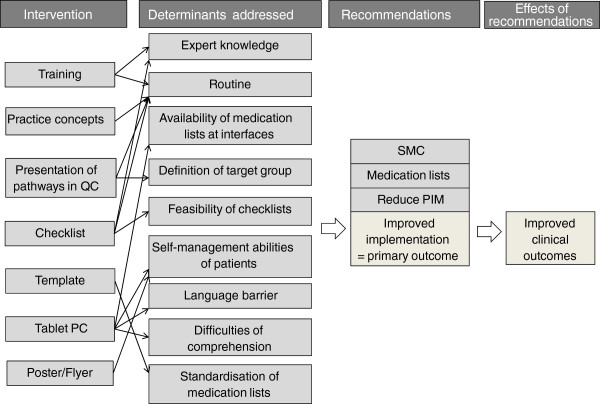
Methods/design: The study is designed as a cluster randomized controlled trial with primary care practices of general practitioners (GPs) who are organized in quality circles. Quality circles will be the unit of randomization with a 1:1 ratio. Follow-up time is 6 months. GPs and healthcare assistants in the intervention group will receive training on medication management. Each GP will create a tailored concept of how to implement the three recommendations into his/her practice. Evidence-based checklists for medication counselling and medication reviews will be provided for physicians. A tablet PC with an interactive educational tool and information leaflets will be provided for use by patients to inform about the necessity of continuous medication management. Control practices will not receive special training and will provide care as usual. Primary outcome is the degree of implementation of the three recommendations, which will be measured using a prespecified set of indicators. Additionally, the PIM prescription rate, patient activation, patients' beliefs about medicine, medication adherence and patients' social support will be measured.
Discussion: This study will contribute knowledge about the feasibility of implementing recommendations for managing patients with polypharmacy in primary care practices. Additionally, this study will contribute knowledge about methods for tailoring of implementation interventions.
Trial registration: Clinicaltrials.gov ISRCTN34664024.
Figures
References
-
- Gnjidic D, Hilmer SN, Blyth FM, Naganathan V, Waite L, Seibel MJ, McLachlan AJ, Cumming RG, Handelsman DJ, Le Couteur DG. Polypharmacy cutoff and outcomes: five or more medicines were used to identify community-dwelling older men at risk of different adverse outcomes. J Clin Epidemiol. 2012;65:989–995. doi: 10.1016/j.jclinepi.2012.02.018. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
