

Tardive dyskinesia: therapeutic options for an increasingly common disorder
- PMID: 24310603
- PMCID: PMC3899488
- DOI: 10.1007/s13311-013-0222-5
Tardive dyskinesia: therapeutic options for an increasingly common disorder
Abstract
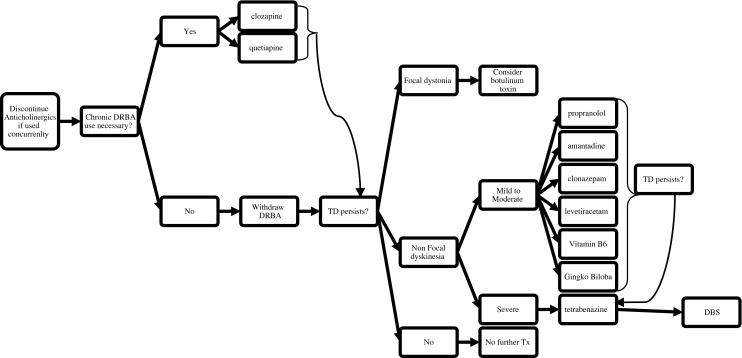
Tardive dyskinesia (TD) is a serious, often disabling, movement disorder that is caused by medications that block dopamine receptors (i.e., neuroleptics, anti-emetics). There is currently no standard treatment approach for physicians confronted with such patients. This may be the result of notions that TD is disappearing because of the switch to second-generation antipsychotic agents and that it is largely reversible. In this article we demonstrate that second-generation antipsychotics do, indeed, cause TD and, in fact, the frequency is likely higher than expected because of growing off-label uses and a tripling of prescriptions written in the last 10 years. In addition, studies demonstrate that TD actually remits in only a minority of patients when these drugs are withdrawn. Furthermore, neuroleptic agents are often utilized to treat TD, despite prolonged exposure being a risk factor for irreversibility. The outcome of these trends is a growing population afflicted with TD. We review non-neuroleptic agents that have shown positive results in small, early-phase, blinded trials, including tetrabenazine, amantadine, levetiracetam, piracetam, clonazepam, propranolol, vitamin B6, and Ginkgo biloba. Other options, such as botulinum toxin and deep brain stimulation, will also be discussed, and a suggested treatment algorithm is provided. While these agents are reasonable treatment options at this time there is a need, with a concerted effort between neurology and psychiatry, for full-scale drug development, including multicenter, randomized, blinded trials to confirm the effectiveness of the agents that were positive in phase 2 trials and the development of newer ones.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
