

Association between AKI and long-term renal and cardiovascular outcomes in United States veterans
- PMID: 24311708
- PMCID: PMC3944753
- DOI: 10.2215/CJN.02440213
Association between AKI and long-term renal and cardiovascular outcomes in United States veterans
Abstract
Background and objectives: AKI is associated with major adverse kidney events (MAKE): death, new dialysis, and worsened renal function. CKD (arising from worsened renal function) is associated with a higher risk of major adverse cardiac events (MACE): myocardial infarction (MI), stroke, and heart failure. Therefore, the study hypothesis was that veterans who develop AKI during hospitalization for an MI would be at higher risk of subsequent MACE and MAKE.
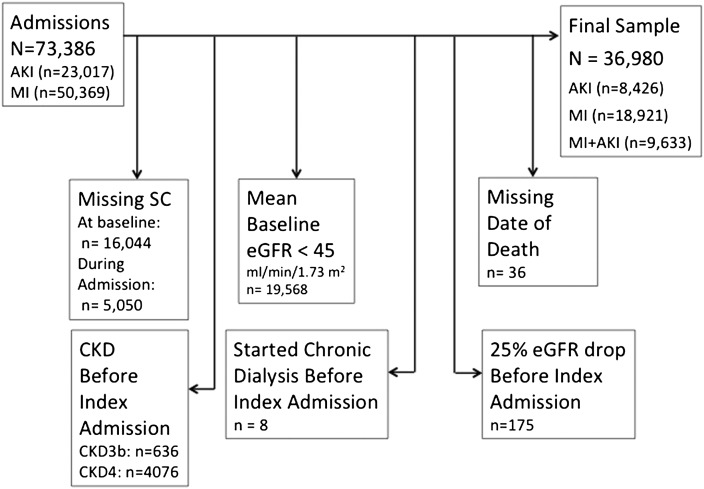
Design, setting, participants, & measurements: Patients in the Veterans Affairs (VA) database who had a discharge diagnosis with International Classification of Diseases, Ninth Revision, code of 584.xx (AKI) or 410.xx (MI) and were admitted to a VA facility from October 1999 through December 2005 were selected for analysis. Three groups of patients were created on the basis of the index admission diagnosis and serum creatinine values: AKI, MI, or MI with AKI. Patients with mean baseline estimated GFR<45 ml/min per 1.73 m(2) were excluded. The primary outcomes assessed were mortality, MAKE, and MACE during the study period (maximum of 6 years). The combination of MAKE and MACE-major adverse renocardiovascular events (MARCE)-was also assessed.
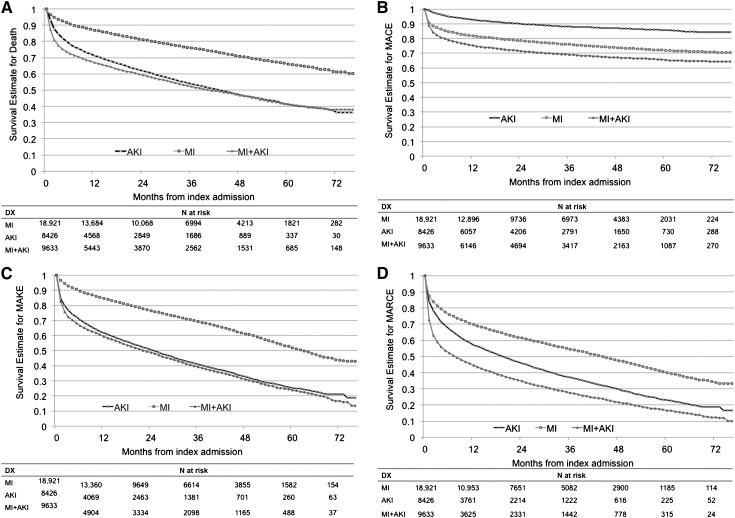
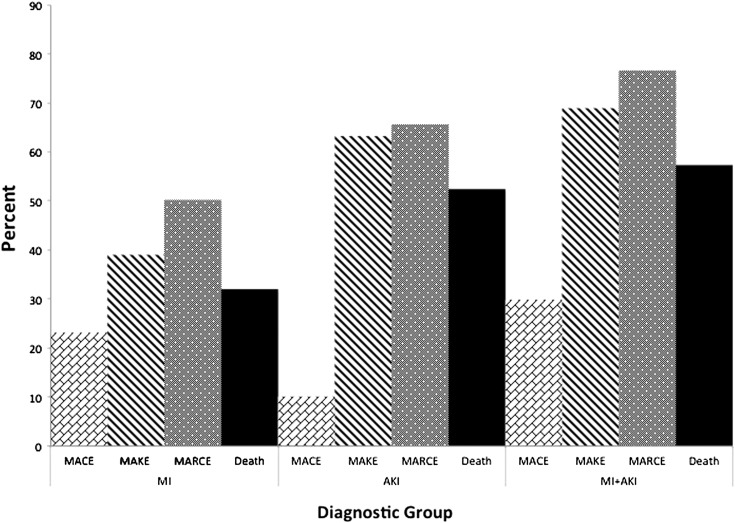
Results: A total of 36,980 patients were available for analysis. Mean age±SD was 66.8±11.4 years. The most deaths occurred in the MI+AKI group (57.5%), and the fewest (32.3%) occurred in patients with an uncomplicated MI admission. In both the unadjusted and adjusted time-to-event analyses, patients with AKI and AKI+MI had worse MARCE outcomes than those who had MI alone (adjusted hazard ratios, 1.37 [95% confidence interval, 1.32 to 1.42] and 1.92 [1.86 to 1.99], respectively).
Conclusions: Veterans who develop AKI in the setting of MI have worse long-term outcomes than those with AKI or MI alone. Veterans with AKI alone have worse outcomes than those diagnosed with an MI in the absence of AKI.
Figures
Comment in
-
AKI: not just a short-term problem?Clin J Am Soc Nephrol. 2014 Mar;9(3):435-6. doi: 10.2215/CJN.00500114. Epub 2014 Feb 13. Clin J Am Soc Nephrol. 2014. PMID: 24526743 Free PMC article. No abstract available.
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators : Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 294: 813–818, 2005 - PubMed
-
- Waikar SS, Liu KD, Chertow GM: Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol 3: 844–861, 2008 - PubMed
-
- Waikar SS, Curhan GC, Wald R, McCarthy EP, Chertow GM: Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol 17: 1143–1150, 2006 - PubMed
-
- Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, Himmelfarb J, Collins AJ: Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol 17: 1135–1142, 2006 - PubMed
-
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J: Independent association between acute renal failure and mortality following cardiac surgery. Am J Med 104: 343–348, 1998 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
