

The effect of dosing regimens on the antimalarial efficacy of dihydroartemisinin-piperaquine: a pooled analysis of individual patient data
- PMID: 24311989
- PMCID: PMC3848996
- DOI: 10.1371/journal.pmed.1001564
The effect of dosing regimens on the antimalarial efficacy of dihydroartemisinin-piperaquine: a pooled analysis of individual patient data
Erratum in
- PLoS Med. 2013 Dec;10(12). doi:10.1371/annotation/3db421e4-3e27-4442-8092-2ad1b778f371
Abstract
Background: Dihydroartemisinin-piperaquine (DP) is increasingly recommended for antimalarial treatment in many endemic countries; however, concerns have been raised over its potential under dosing in young children. We investigated the influence of different dosing schedules on DP's clinical efficacy.
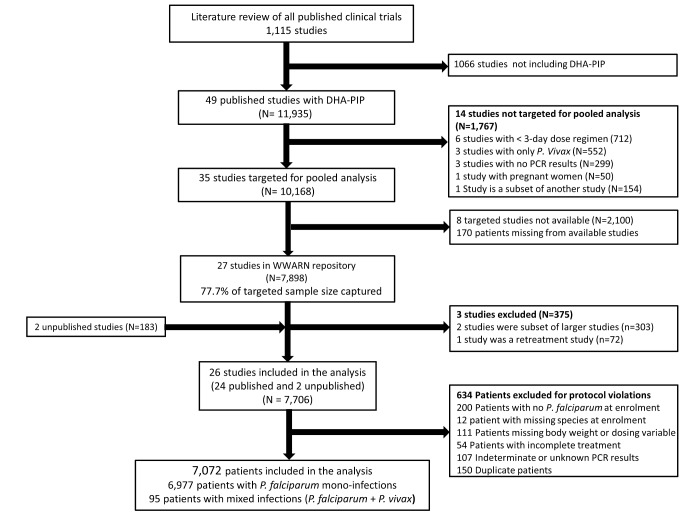
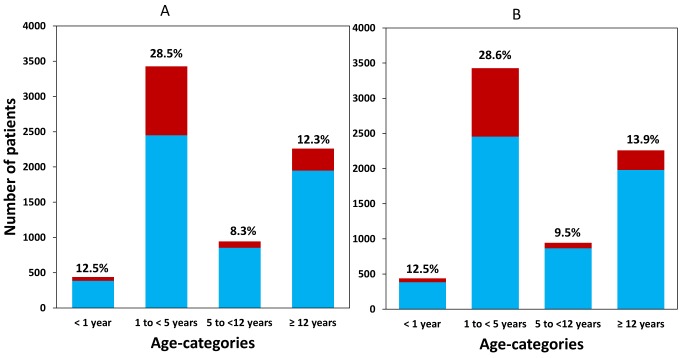
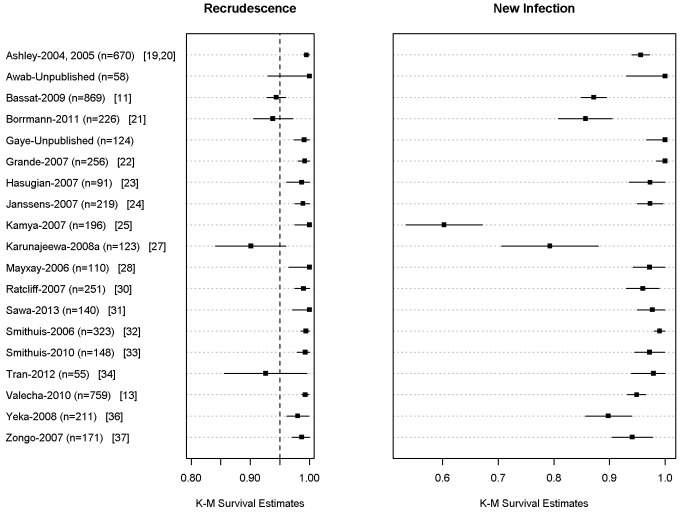
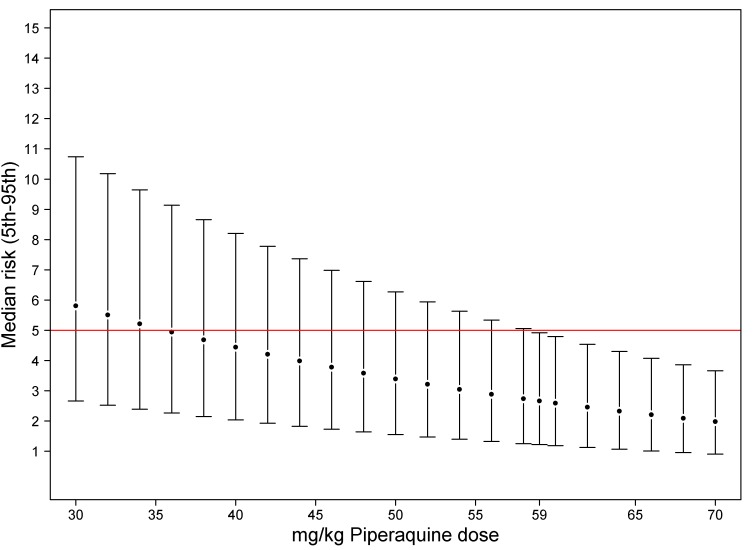
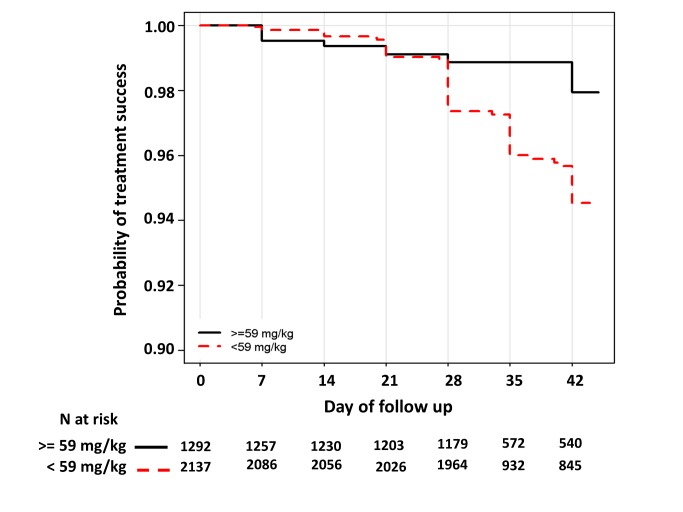
Methods and findings: A systematic search of the literature was conducted to identify all studies published between 1960 and February 2013, in which patients were enrolled and treated with DP. Principal investigators were approached and invited to share individual patient data with the WorldWide Antimalarial Resistance Network (WWARN). Data were pooled using a standardised methodology. Univariable and multivariable risk factors for parasite recrudescence were identified using a Cox's regression model with shared frailty across the study sites. Twenty-four published and two unpublished studies (n = 7,072 patients) were included in the analysis. After correcting for reinfection by parasite genotyping, Kaplan-Meier survival estimates were 97.7% (95% CI 97.3%-98.1%) at day 42 and 97.2% (95% CI 96.7%-97.7%) at day 63. Overall 28.6% (979/3,429) of children aged 1 to 5 years received a total dose of piperaquine below 48 mg/kg (the lower limit recommended by WHO); this risk was 2.3-2.9-fold greater compared to that in the other age groups and was associated with reduced efficacy at day 63 (94.4% [95% CI 92.6%-96.2%], p<0.001). After adjusting for confounding factors, the mg/kg dose of piperaquine was found to be a significant predictor for recrudescence, the risk increasing by 13% (95% CI 5.0%-21%) for every 5 mg/kg decrease in dose; p = 0.002. In a multivariable model increasing the target minimum total dose of piperaquine in children aged 1 to 5 years old from 48 mg/kg to 59 mg/kg would halve the risk of treatment failure and cure at least 95% of patients; such an increment was not associated with gastrointestinal toxicity in the ten studies in which this could be assessed.
Conclusions: DP demonstrates excellent efficacy in a wide range of transmission settings; however, treatment failure is associated with a lower dose of piperaquine, particularly in young children, suggesting potential for further dose optimisation.
Conflict of interest statement
EAA has worked as an investigator on studies of dihydroartemisinin-piperaquine sponsored by both Holley-Cotec and Medicines for Malaria Venture. EAA and FN have received research funding from Holley-Cotec. KIB serves as a member of a number of malaria-related World Health Organization committees, including the Malaria Chemotherapy Technical Expert Group. KIB is a recipient of a research grant from the Medicines for Malaria Venture and is a sub-recipient of grants from the Bill & Melinda Gates Foundation. QB has received speaker fees and travel grants from Sigma Tau. UDA has received research funding and several travel grants from Sigma Tau; UDA has been a consultant for Sigma Tau on dihydroartemisinin-piperaquine. CMenéndez and NJW are members of the Editorial Board of
Figures
Comment in
-
Artemisinin combination therapy: a good antimalarial, but is the dose right?PLoS Med. 2013 Dec;10(12):e1001565. doi: 10.1371/journal.pmed.1001565. Epub 2013 Dec 3. PLoS Med. 2013. PMID: 24348204 Free PMC article.
References
-
- Carneiro I, Roca-Feltrer A, Griffin JT, Smith L, Tanner M, et al. (2010) Age-patterns of malaria vary with severity, transmission intensity and seasonality in sub-Saharan Africa: a systematic review and pooled analysis. PLoS One 5: e8988 doi: 10.1371/journal.pone.0008988 - DOI - PMC - PubMed
-
- Price R, Luxemburger C, van Vugt M, Nosten F, Kham A, et al. (1998) Artesunate and mefloquine in the treatment of uncomplicated multidrug-resistant hyperparasitaemic falciparum malaria. Trans R Soc Trop Med Hyg 92: 207–211. - PubMed
-
- WHO (2010) Guidelines for the treatment of malaria, second edition. 2012. Available: http://whqlibdoc.who.int/publications/2010/9789241547925_eng.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
