

Estimating influenza deaths in Canada, 1992-2009
- PMID: 24312225
- PMCID: PMC3842334
- DOI: 10.1371/journal.pone.0080481
Estimating influenza deaths in Canada, 1992-2009
Abstract
Background: Poisson regression modelling has been widely used to estimate the disease burden attributable to influenza, though not without concerns that some of the excess burden could be due to other causes. This study aims to provide annual estimates of the mortality and hospitalization burden attributable to both seasonal influenza and the 2009 A/H1N1 pandemic influenza for Canada, and to discuss issues related to the reliability of these estimates.
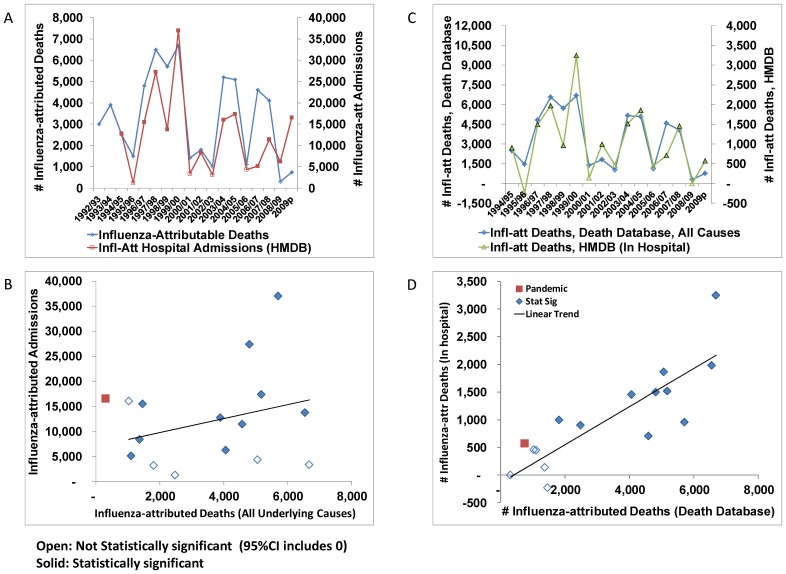
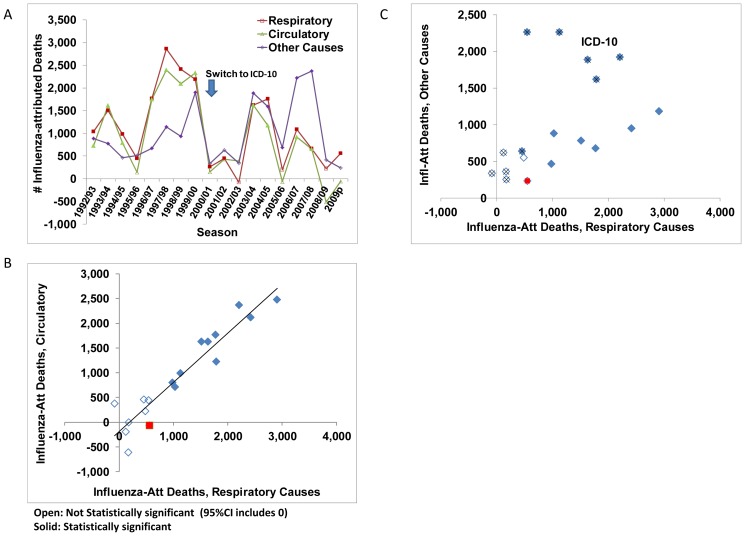
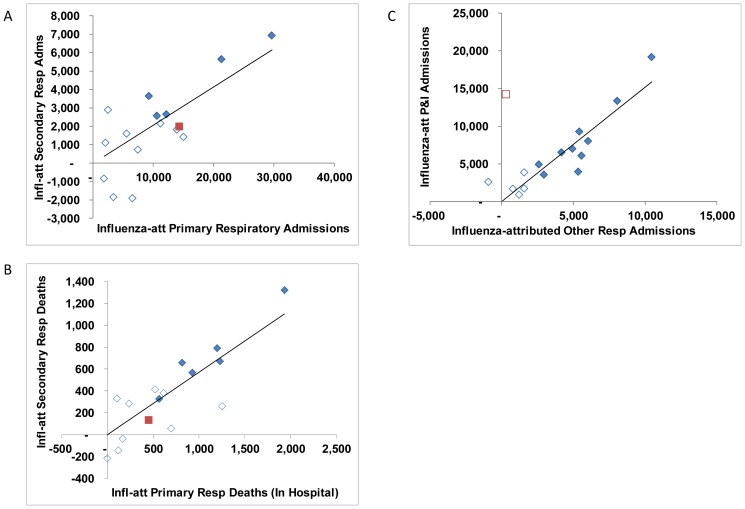
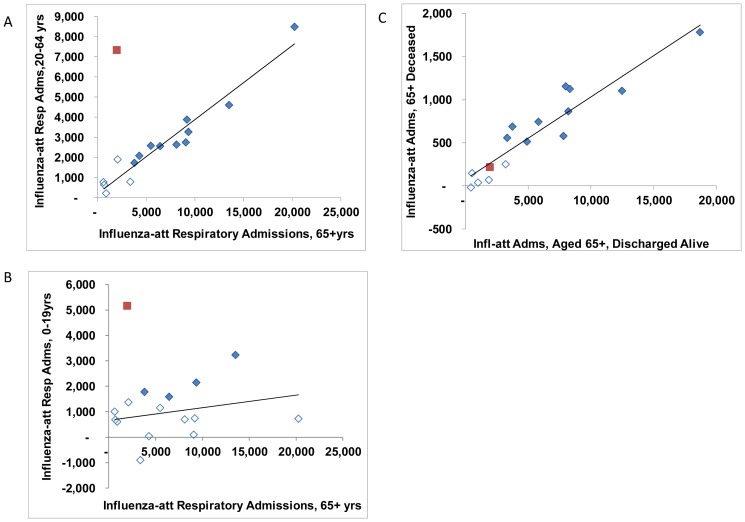
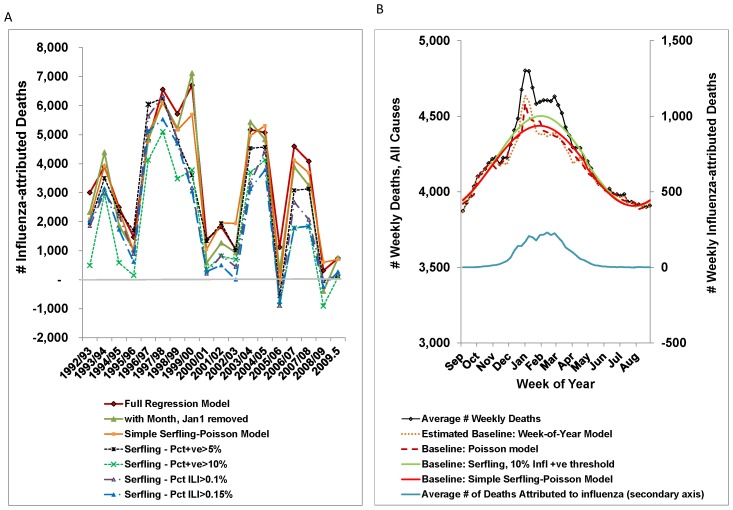
Methods: Weekly time-series for all-cause mortality and regression models were used to estimate the number of deaths in Canada attributable to influenza from September 1992 to December 2009. To assess their robustness, the annual estimates derived from different parameterizations of the regression model for all-cause mortality were compared. In addition, the association between the annual estimates for mortality and hospitalization by age group, underlying cause of death or primary reason for admission and discharge status is discussed.
Results: The crude influenza-attributed mortality rate based on all-cause mortality and averaged over 17 influenza seasons prior to the 2009 A/H1N1 pandemic was 11.3 (95%CI, 10.5 - 12.1) deaths per 100 000 population per year, or an average of 3,500 (95%CI, 3,200 - 3,700) deaths per year attributable to seasonal influenza. The estimated annual rates ranged from undetectable at the ecological level to more than 6000 deaths per year over the three A/Sydney seasons. In comparison, we attributed an estimated 740 deaths (95%CI, 350-1500) to A(H1N1)pdm09. Annual estimates from different model parameterizations were strongly correlated, as were estimates for mortality and morbidity; the higher A(H1N1)pdm09 burden in younger age groups was the most notable exception.
Interpretation: With the exception of some of the Serfling models, differences in the ecological estimates of the disease burden attributable to influenza were small in comparison to the variation in disease burden from one season to another.
Conflict of interest statement
Figures
References
-
- Thompson WW, Ridenhour BL, Barile JP, Shay DK (2012) Time-series analyses of count data to estimate the burden of seasonal infectious diseases. Epidemiology 23: 839–842. - PubMed
-
- World Health Organization (2009) Comparing deaths from pandemic and seasonal influenza: Pandemic (H1N1) 2009 briefing note 20. Available: http://www.who.int/csr/disease/swineflu/notes/briefing_20091222/en/index... via the Internet. Accessed 26 April 2010.
-
- Schanzer DL, Langley JM, Tam TWS (2008) Co-morbidities associated with influenza-attributed mortality, 1994–2000, Canada. Vaccine 26: 4697–703. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
