

Quality along the continuum: a health facility assessment of intrapartum and postnatal care in Ghana
- PMID: 24312265
- PMCID: PMC3842335
- DOI: 10.1371/journal.pone.0081089
Quality along the continuum: a health facility assessment of intrapartum and postnatal care in Ghana
Erratum in
-
Correction: Quality along the Continuum: A Health Facility Assessment of Intrapartum and Postnatal Care in Ghana.PLoS One. 2015 Oct 20;10(10):e0141517. doi: 10.1371/journal.pone.0141517. eCollection 2015. PLoS One. 2015. PMID: 26485127 Free PMC article. No abstract available.
Abstract
Objective: To evaluate quality of routine and emergency intrapartum and postnatal care using a health facility assessment, and to estimate "effective coverage" of skilled attendance in Brong Ahafo, Ghana.
Methods: We conducted an assessment of all 86 health facilities in seven districts in Brong Ahafo. Using performance of key signal functions and the availability of relevant drugs, equipment and trained health professionals, we created composite quality categories in four dimensions: routine delivery care, emergency obstetric care (EmOC), emergency newborn care (EmNC) and non-medical quality. Linking the health facility assessment to surveillance data we estimated "effective coverage" of skilled attendance as the proportion of births in facilities of high quality.
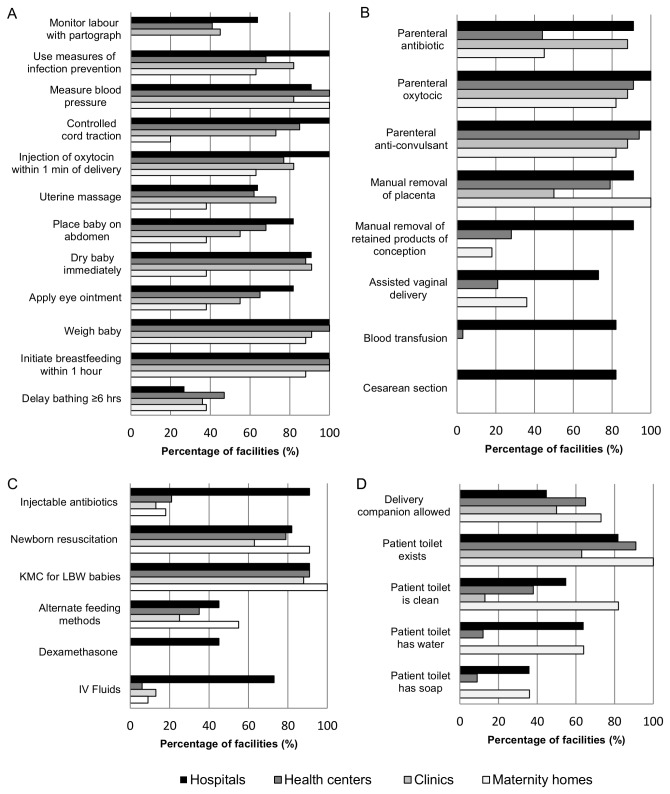
Findings: Delivery care was offered in 64/86 facilities; only 3-13% fulfilled our requirements for the highest quality category in any dimension. Quality was lowest in the emergency care dimensions, with 63% and 58% of facilities categorized as "low" or "substandard" for EmOC and EmNC, respectively. This implies performing less than four EmOC or three EmNC signal functions, and/or employing less than two skilled health professionals, and/or that no health professionals were present during our visit. Routine delivery care was "low" or "substandard" in 39% of facilities, meaning 25/64 facilities performed less than six routine signal functions and/or had less than two skilled health professionals and/or less than one midwife. While 68% of births were in health facilities, only 18% were in facilities with "high" or "highest" quality in all dimensions.
Conclusion: Our comprehensive facility assessment showed that quality of routine and emergency intrapartum and postnatal care was generally low in the study region. While coverage with facility delivery was 68%, we estimated "effective coverage" of skilled attendance at 18%, thus revealing a large "quality gap." Effective coverage could be a meaningful indicator of progress towards reducing maternal and newborn mortality.
Conflict of interest statement
Figures


References
-
- Lawn JE, Lee AC, Kinney M, Sibley L, Carlo WA, et al. (2009) Two million intrapartum-related stillbirths and neonatal deaths: where, why, and what can be done? Int J Gynaecol Obstet 107 Suppl 1: S5-18, S19 - PubMed
-
- World Health Organization (WHO) (2009) Monitoring Emergency Obstetric Care. A Handbook. Available: <ext-link xmlns:xlink="http://www.w3.org/1999/xlink" ext-link-type="uri" xlink:href="http://www.who.int/reproductivehealth/publications/monitoring/9789241547..."><underline>http://www.who.int/reproductivehealth/publications/monitoring/9789241547...</underline></ext-link>. Accessed August 17 2012
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
