

The potential of antimicrobials to induce thrombocytopenia in critically ill patients: data from a randomized controlled trial
- PMID: 24312305
- PMCID: PMC3842947
- DOI: 10.1371/journal.pone.0081477
The potential of antimicrobials to induce thrombocytopenia in critically ill patients: data from a randomized controlled trial
Abstract
Background: Antimicrobial-induced thrombocytopenia is frequently described in the literature among critically ill patients. Several antimicrobials have been implicated, although experimental evidence to demonstrate causality is limited. We report, using a randomized trial, the potential of antimicrobials to induce thrombocytopenia.
Methods: Randomized trial allocated patients to antimicrobial treatment according to standard- of-care (SOC group) or drug-escalation in case of procalcitonin increases (high-exposure group). Patients were followed until death or day 28. Thrombocytopenia defined as absolute (platelet count ≤ 100 x 109/L) or relative (≥ 20% decrease in platelet count). Analyses were performed in the two randomized groups and as a merged cohort.
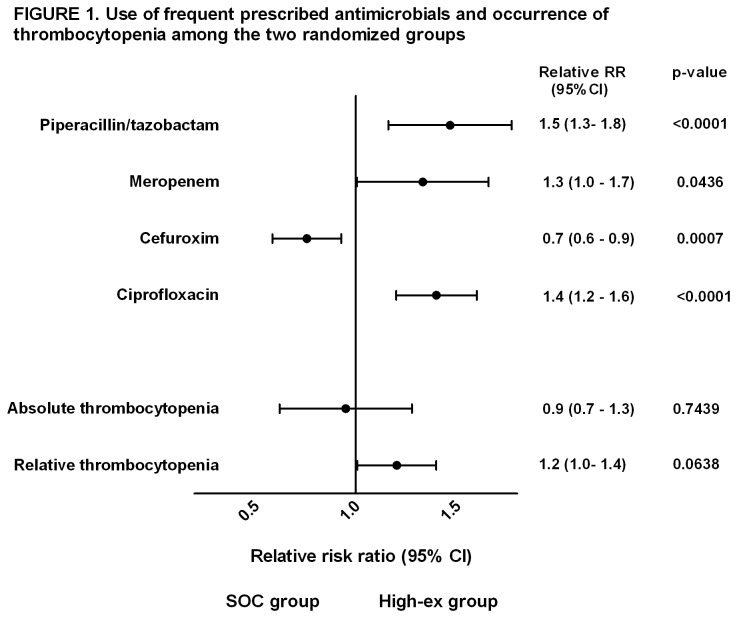
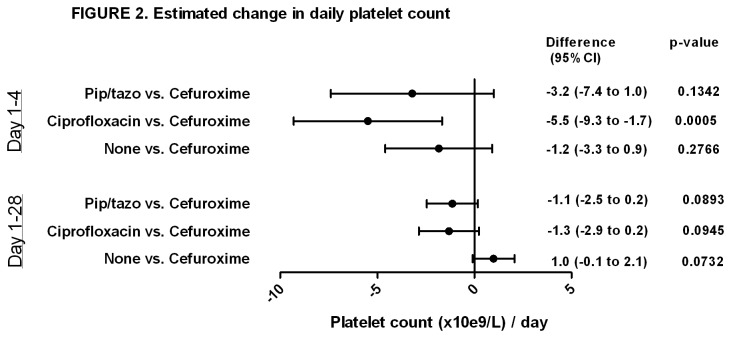
Results: Of the 1147 patients with platelet data available, 18% had absolute thrombocytopenia within the first 24 hours after admission to intensive care unit and additional 17% developed this complication during follow-up; 57% developed relative thrombocytopenia during follow-up. Absolute and relative thrombocytopenia day 1-4 was associated with increased mortality (HR: 1.67 [95% CI: 1.30 to 2.14]; 1.71 [95% CI: 1.30 to 2.30], P<0.0001, respectively). Patients in the high-exposure group received more antimicrobials including piperacillin/tazobactam, meropenem and ciprofloxacin compared with the SOC group, whereas cefuroxime was used more frequently in the SOC group (p<0.05). Risk of absolute and relative thrombocytopenia (RR: 0.9 [0.7-1.3], p=0.7439; 1.2 [1.0-1.4], p=0.06; respectively), as well as absolute platelet count (daily difference, high-exposure vs. SOC -1.7 [-3.8-0.5], p=0.14) was comparable between groups. In observational analyses, use of ciprofloxacin and piperacillin/tazobactam predicted risk of relative thrombocytopenia (vs. cefuroxime, RR: 2.08 [1.48-2.92]; 1.44 [1.10-1.89], respectively), however only ciprofloxacin were associated with a reduction in absolute platelet count (p=0.0005).
Conclusion: High exposure to broad-spectrum antimicrobials does not result in a reduction in thrombocytopenia in critically ill patients. However, single use of ciprofloxacin, and less so piperacillin/tazobactam, may contribute to a lower platelet count.
Trial registration: ClinicalTrials.gov NCT00271752 http://clinicaltrials.gov/ct2/show/NCT00271752.
Conflict of interest statement
Figures
References
-
- Thiolliere F, Serre-Sapin AF, Reignier J, Benedit M, Constantin JM et al. (2013) Epidemiology and outcome of thrombocytopenic patients in the intensive care unit: results of a prospective multicenter study. Intensive Care Med 39: 1460-1468. doi:10.1007/s00134-013-2963-3. PubMed: 23740274. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
