

Anti-remodeling effects of rapamycin in experimental heart failure: dose response and interaction with angiotensin receptor blockade
- PMID: 24312548
- PMCID: PMC3849273
- DOI: 10.1371/journal.pone.0081325
Anti-remodeling effects of rapamycin in experimental heart failure: dose response and interaction with angiotensin receptor blockade
Abstract
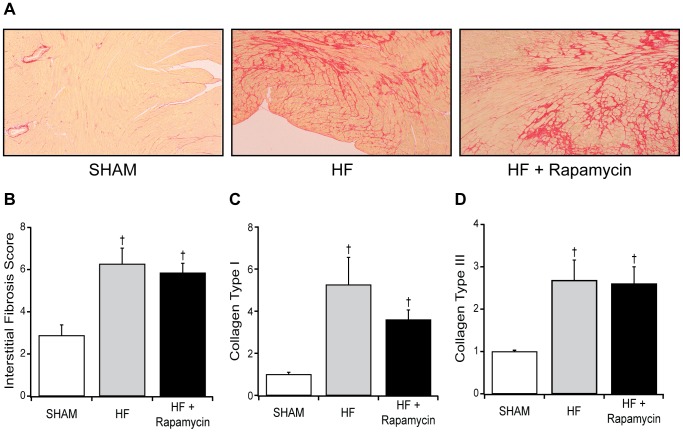
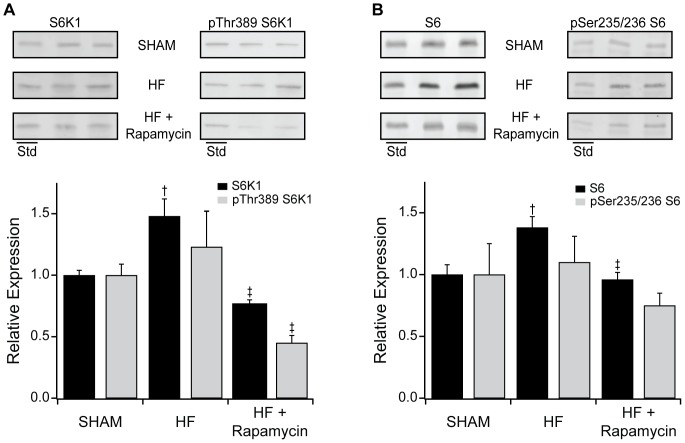
While neurohumoral antagonists improve outcomes in heart failure (HF), cardiac remodeling and dysfunction progress and outcomes remain poor. Therapies superior or additive to standard HF therapy are needed. Pharmacologic mTOR inhibition by rapamycin attenuated adverse cardiac remodeling and dysfunction in experimental heart failure (HF). However, these studies used rapamycin doses that produced blood drug levels targeted for primary immunosuppression in human transplantation and therefore the immunosuppressive effects may limit clinical translation. Further, the relative or incremental effect of rapamycin combined with standard HF therapies targeting upstream regulators of cardiac remodeling (neurohumoral antagonists) has not been defined. Our objectives were to determine if anti-remodeling effects of rapamycin were preserved at lower doses and whether rapamycin effects were similar or additive to a standard HF therapy (angiotensin receptor blocker (losartan)). Experimental murine HF was produced by transverse aortic constriction (TAC). At three weeks post-TAC, male mice with established HF were treated with placebo, rapamycin at a dose producing immunosuppressive drug levels (target dose), low dose (50% target dose) rapamycin, losartan or rapamycin + losartan for six weeks. Cardiac structure and function (echocardiography, catheterization, pathology, hypertrophic and fibrotic gene expression profiles) were assessed. Downstream mTOR signaling pathways regulating protein synthesis (S6K1 and S6) and autophagy (LC3B-II) were characterized. TAC-HF mice displayed eccentric hypertrophy, systolic dysfunction and pulmonary congestion. These perturbations were attenuated to a similar degree by oral rapamycin doses achieving target (13.3±2.1 ng/dL) or low (6.7±2.5 ng/dL) blood levels. Rapamycin treatment decreased mTOR mediated regulators of protein synthesis and increased mTOR mediated regulators of autophagy. Losartan monotherapy did not attenuate remodeling, whereas Losartan added to rapamycin provided no incremental benefit over rapamycin alone. These data lend support to investigation of low dose rapamycin as a novel therapy in human HF.
Conflict of interest statement
Figures





References
-
- Hunt SA, American College of Cardiology, American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure) (2005) ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 46: e1–e82 10.1016/j.jacc.2005.08.022 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
