

Sialyl Lewis X as a predictor of skip N2 metastasis in clinical stage IA non-small cell lung cancer
- PMID: 24313932
- PMCID: PMC4029375
- DOI: 10.1186/1477-7819-11-309
Sialyl Lewis X as a predictor of skip N2 metastasis in clinical stage IA non-small cell lung cancer
Abstract
Background: Radical segmentectomy has been performed for small-sized non-small cell lung cancer (NSCLC). However, underestimation of mediastinal lymph node metastasis in the absence of hilar or interlobar metastasis (skip N2) affects surgical strategy. Our aim was to investigate preoperative and intraoperative predictors of skip N2 in clinical stage (c-stage) IA NSCLC.
Methods: From 1998 to 2011, 279 patients (155 men and 124 women) with c-stage IA NSCLC (230 pN0, 17 pN1, 12 skip N2, 20 non-skip N2) underwent systematic lobectomy (R0 resection) at our institute. We compared preoperative serum concentrations of carcinoembryonic antigen, cytokeratin 19 fragment, sialyl Lewis X (SLX), and pre- and intraoperative clinicopathological features of pN0 and skip N2 patients. Receiver operator characteristic (ROC) curve analysis was performed to distinguish between the two patient groups.
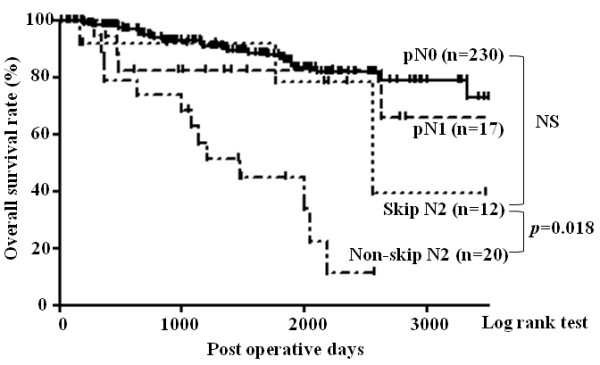
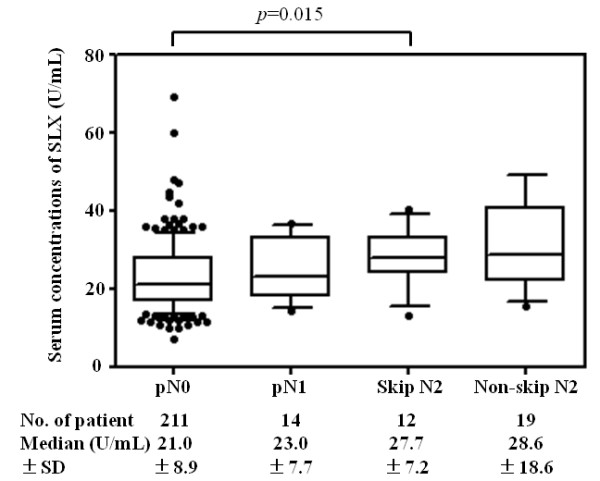
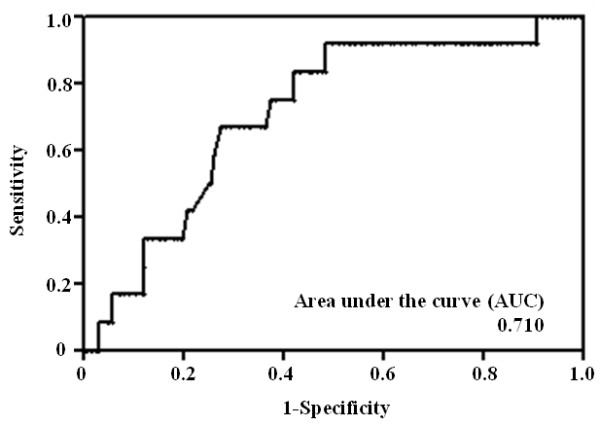
Results: The 5-year survival rate of skip N2 patients was 78.6%, higher than that of non-skip N2 patients (44.9%), and not significantly different than that of pN0 (86.7%) or pN1 patients (82.4%). The mean serum SLX concentration in skip N2 patients (28.0 U/ml) was elevated compared to that in pN0 patients (22.9 U/ml). In ROC analysis of SLX, the area under the curve was 0.710, and the optimal cut-off value was 21.4 U/ml (sensitivity, 91.7%; specificity, 51.7%). In multivariate analysis, SLX was an independent predictor of skip N2 in patients with c-stage IA NSCLC (odds ratio, 9.43; p = 0.006).
Conclusions: Skip N2 metastasis is common in patients with c-stage IA NSCLC with high serum SLX, and lobectomy with complete dissection of hilar and mediastinal lymph nodes should remain the standard surgical procedure for these cases.
Figures
References
-
- Goldstraw P, Crowley JJ. IASLC International Staging Project. The International Association for the Study of Lung Cancer International Staging Project on Lung Cancer. J Thorac Oncol. 2006;11:281–286. doi: 10.1097/01243894-200605000-00002. - DOI
-
- Naruke T, Tsuchiya R, Kondo H, Nakayama H, Asamura H. Lymph node sampling in lung cancer: how should it be done? Eur J Cardiothorac Surg. 1999;11:S17–S24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
