

Use of health care services by people with mental illness: secondary data from three statutory health insurers and the German Statutory Pension Insurance Scheme
- PMID: 24314623
- PMCID: PMC3859909
- DOI: 10.3238/arztebl.2013.0799
Use of health care services by people with mental illness: secondary data from three statutory health insurers and the German Statutory Pension Insurance Scheme
Abstract
Background: A discipline- and sector-specific analysis of health-care utilization by persons with mental illness in Germany is an indispensable aid to planning for the provision of adequate basic care.
Method: Secondary data from three statutory health insurers and the German Statutory Pension Insurance Scheme for the period 2005-2007 were evaluated to identify insurees with mental illness (ICD-10 diagnosis groups F0-F5).
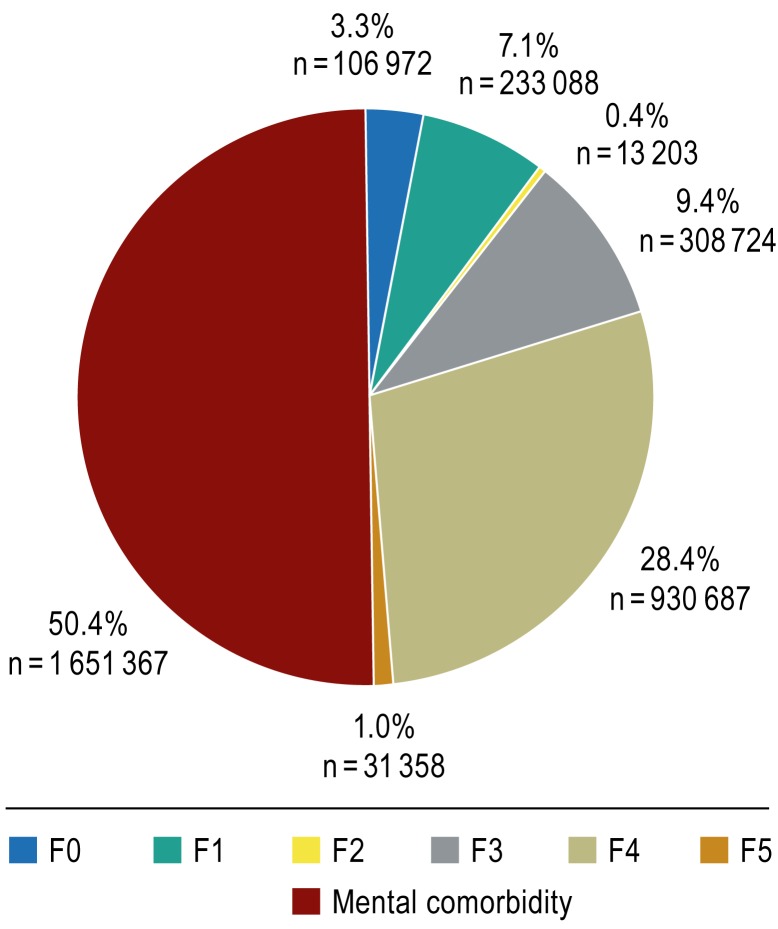
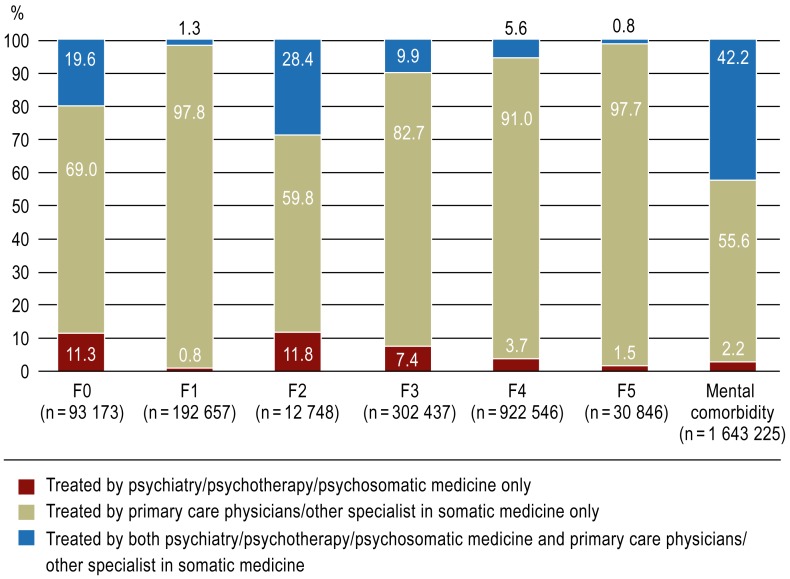
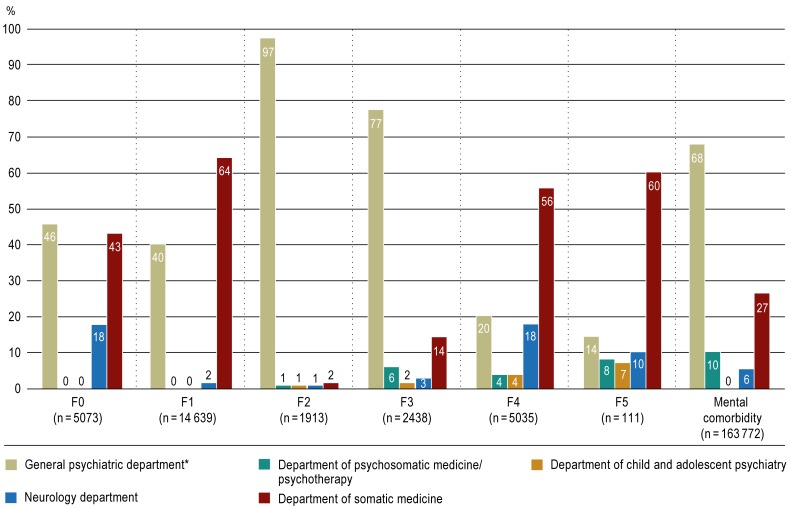
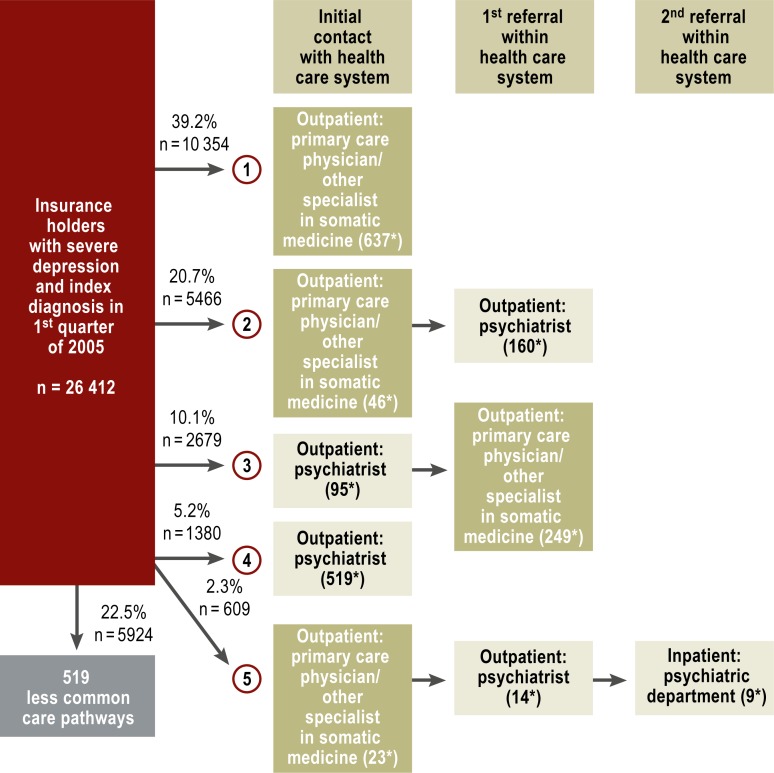
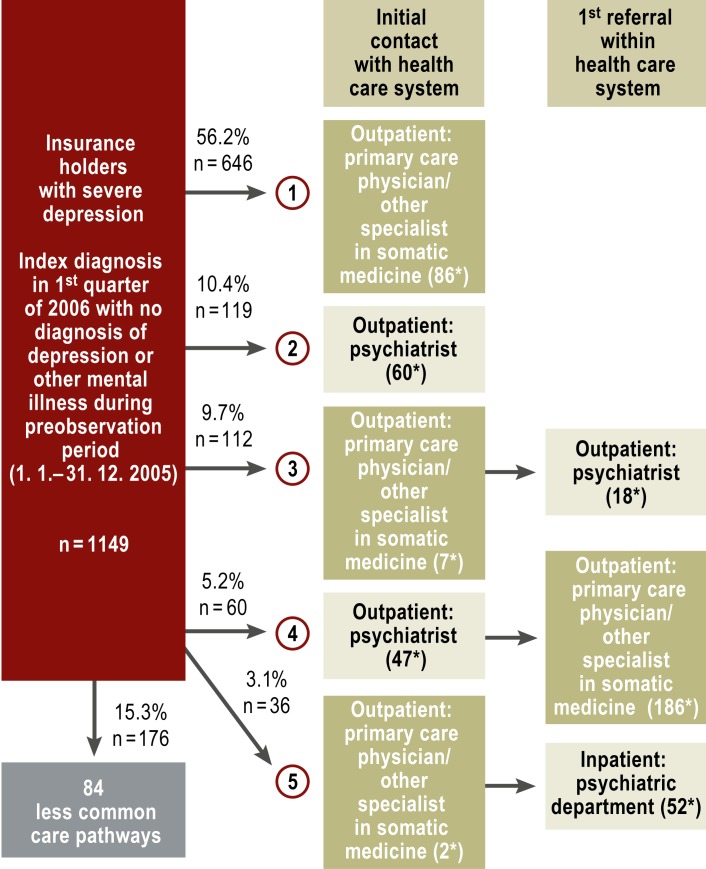
Results: In the period 2005-2007, 3.28 million (33%) of 9.92 million insurees had at least one contact with the health-care system in which a mental disorder was diagnosed. 50.4% (1,651,367) of these insurees had at least two mental disorders. Nearly all (98.8%) of the insurees with a psychiatric index diagnosis had at least one somatic diagnosis coded as well. 95.7% of treatments were provided in the outpatient setting. Somatic medical specialties provided the majority of treatments both in ambulatory care and in the hospital. For example, 77.5% of persons with severe depression were treated with five kinds of treatment that were provided exclusively by primary care physicians and other specialists in somatic medicine in private practice, sometimes in combination with psychiatric treatment or psychotherapy.
Conclusion: There was a high degree of comorbidity of mental and somatic illness. The fact that the vast majority of treatment was provided in the outpatient setting implies that cooperation across health-care sectors and disciplines should be reinforced, and that measures should be taken to ensure the adequate delivery of basic psychiatric care by primary care physicians.
Figures
Comment in
-
Waiting times are too long.Dtsch Arztebl Int. 2014 Apr 11;111(15):271. doi: 10.3238/arztebl.2014.0271a. Dtsch Arztebl Int. 2014. PMID: 24776612 Free PMC article. No abstract available.
-
Diagnoses as "currency".Dtsch Arztebl Int. 2014 Apr 11;111(15):271. doi: 10.3238/arztebl.2014.0271b. Dtsch Arztebl Int. 2014. PMID: 24776613 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2014 Apr 11;111(15):271-2. doi: 10.3238/arztebl.2014.0271c. Dtsch Arztebl Int. 2014. PMID: 24776614 Free PMC article. No abstract available.
References
-
- DRAK- Unternehmen Leben. www.presse.dak.de/ps.nsf/Show/03AF73C39B7227B0C12576BF004C8490/$File/DAK.... Hamburg: 2010. DAK-Gesundheitsreport 2010. last accessed 17. October 2013.
-
- Dannenberg A, Hofmann J, Kaldybajewa K, Kruse E. Rentenzugang 2009: Weiterer Anstieg der Zugänge in Erwerbsminderungsrenten wegen psychischer Erkrankungen. RV aktuell. 2009;9:283–293.
-
- Albrecht M, Fürstenberg T, Gottberg A. IGES Institut. Berlin: 2007. Strukturen und Finanzierung der neurologischen und psychiatrischen Versorgung.
-
- Wittchen HU, Jacobi F. Die Versorgungssituation psychischer Störungen in Deutschland. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. 2001;44:993–1000.
-
- Kovess-Masfety V, Alonso J, Brugha TS, Angermeyer MC, Haro JM, Sevilla-Dedieu C and the ESEMeD/MHEDEA 2000 Investigators. Differences in lifetime use of services for mental health problems in six European countries. Psychiat Serv. 2007;58:213–220. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous