

Derivation of a clinical decision instrument to identify adult patients with mild traumatic intracranial hemorrhage at low risk for requiring ICU admission
- PMID: 24314900
- PMCID: PMC3965594
- DOI: 10.1016/j.annemergmed.2013.11.003
Derivation of a clinical decision instrument to identify adult patients with mild traumatic intracranial hemorrhage at low risk for requiring ICU admission
Abstract
Study objective: The objective of this study is to derive a clinical decision instrument with a sensitivity of at least 95% (with upper and lower bounds of the 95% confidence intervals [CIs] within a 5% range) to identify adult emergency department patients with mild traumatic intracranial hemorrhage who are at low risk for requiring critical care resources during hospitalization and thus may not need admission to the ICU.
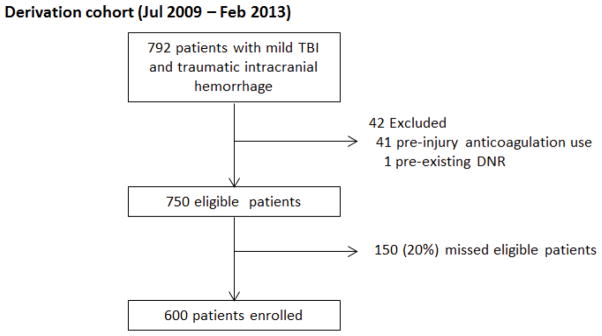
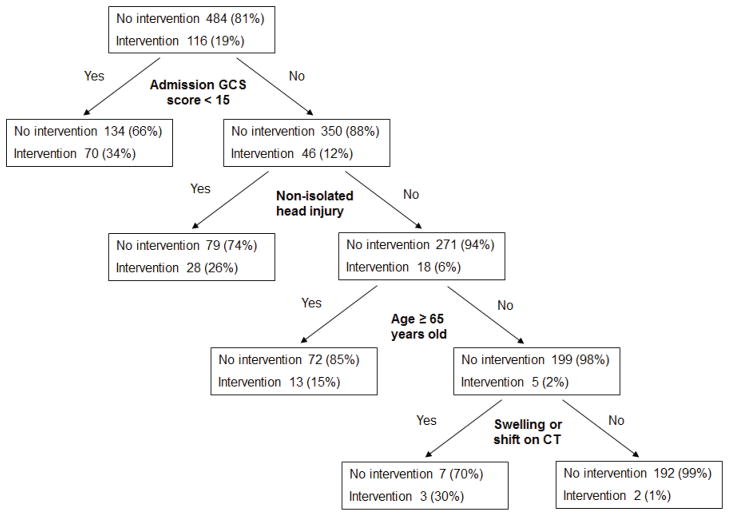
Methods: This was a prospective, observational study of adult patients with mild traumatic intracranial hemorrhage (initial Glasgow Coma Scale [GCS] score 13 to 15, with traumatic intracranial hemorrhage) presenting to a Level I trauma center from July 2009 to February 2013. The need for ICU admission was defined as the presence of an acute critical care intervention (intubation, neurosurgical intervention, blood product transfusion, vasopressor or inotrope administration, invasive monitoring for hemodynamic instability, urgent treatment for arrhythmia or cardiopulmonary resuscitation, and therapeutic angiography). We derived the clinical decision instrument with binary recursive partitioning (with a misclassification cost of 20 to 1). The accuracy of the decision instrument was compared with the treating physician's (emergency medicine faculty) clinical impression.
Results: A total of 600 patients with mild traumatic intracranial hemorrhage were enrolled; 116 patients (19%) had a critical care intervention. The derived instrument consisted of 4 predictor variables: admission GCS score less than 15, nonisolated head injury, aged 65 years or older, and evidence of swelling or shift on initial cranial computed tomography scan. The decision instrument identified 114 of 116 patients requiring an acute critical care intervention (sensitivity 98.3%; 95% CI 93.9% to 99.5%) if at least 1 variable was present and 192 of 484 patients who did not have an acute critical care intervention (specificity 39.7%; 95% CI 35.4% to 44.1%) if no variables were present. Physician clinical impression was slightly less sensitive (90.1%; 95% CI 83.1% to 94.4%) but overall similar to the clinical decision instrument.
Conclusion: We derived a clinical decision instrument that identifies a subset of patients with mild traumatic intracranial hemorrhage who are at low risk for acute critical care intervention and thus may not require ICU admission. Physician clinical impression had test characteristics similar to those of the decision instrument. Because the results are based on single-center data without a validation cohort, external validation is required.
Copyright © 2013 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
None
Figures
Similar articles
-
A clinical decision rule to predict adult patients with traumatic intracranial haemorrhage who do not require intensive care unit admission.Injury. 2012 Nov;43(11):1827-32. doi: 10.1016/j.injury.2011.07.020. Epub 2011 Aug 11. Injury. 2012. PMID: 21839444 Free PMC article.
-
Medical necessity of routine admission of children with mild traumatic brain injury to the intensive care unit.J Neurosurg Pediatr. 2017 Jun;19(6):668-674. doi: 10.3171/2017.2.PEDS16419. Epub 2017 Apr 7. J Neurosurg Pediatr. 2017. PMID: 28387644
-
Variability of ICU use in adult patients with minor traumatic intracranial hemorrhage.Ann Emerg Med. 2013 May;61(5):509-517.e4. doi: 10.1016/j.annemergmed.2012.08.024. Epub 2012 Sep 27. Ann Emerg Med. 2013. PMID: 23021347 Free PMC article.
-
Risk factors for traumatic intracranial hemorrhage in mild traumatic brain injury patients at the emergency department: a systematic review and meta-analysis.Scand J Trauma Resusc Emerg Med. 2024 Sep 17;32(1):91. doi: 10.1186/s13049-024-01262-6. Scand J Trauma Resusc Emerg Med. 2024. PMID: 39289729 Free PMC article.
-
Management of traumatic intracranial hemorrhage in the emergency department.Emerg Med Pract. 2025 Feb 1;27(2):1-32. Print 2025 Feb. Emerg Med Pract. 2025. PMID: 39836567 Review.
Cited by
-
Long-term neurological outcomes in adults with traumatic intracranial hemorrhage admitted to ICU versus floor.West J Emerg Med. 2015 Mar;16(2):284-90. doi: 10.5811/westjem.2015.1.23356. Epub 2015 Mar 2. West J Emerg Med. 2015. PMID: 25834671 Free PMC article.
-
Prediction of neurosurgical intervention after mild traumatic brain injury using the national trauma data bank.World J Emerg Surg. 2015 Jun 6;10:23. doi: 10.1186/s13017-015-0017-6. eCollection 2015. World J Emerg Surg. 2015. PMID: 26060506 Free PMC article.
-
Patient Admission Preferences and Perceptions.West J Emerg Med. 2015 Sep;16(5):707-14. doi: 10.5811/westjem.2015.7.27458. Epub 2015 Oct 20. West J Emerg Med. 2015. PMID: 26587095 Free PMC article.
-
Reliability of Clinical Assessments in Older Adults With Syncope or Near Syncope.Acad Emerg Med. 2016 Sep;23(9):1014-21. doi: 10.1111/acem.12977. Epub 2016 Sep 6. Acad Emerg Med. 2016. PMID: 27027730 Free PMC article.
-
Hospital admission of older patients with mild traumatic brain injury and traumatic intracranial hemorrhage: is it always necessary?Eur J Trauma Emerg Surg. 2025 Jan 12;51(1):8. doi: 10.1007/s00068-024-02671-z. Eur J Trauma Emerg Surg. 2025. PMID: 39799536 Free PMC article.
References
-
- Marshall LF, Klauber MR. The outcome of severe closed head injury. J Neurosurg. 1991;75:S28–36.
-
- Huynh T, Jacobs DG, Dix S, Sing RF, Miles WS, Thomason MH. Utility of neurosurgical consultation for mild traumatic brain injury. Am Surg. 2006;72(12):1162–5. - PubMed
-
- Sifri ZC, Livingston DH, Lavery RF, Homnick AT, Mosenthal AC, Mohr AM, et al. Value of repeat cranial computed axial tomography scanning in patients with minimal head injury. Am J Surg. 2004;187(3):338–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
