

Clinical value of magnetoencephalographic spike propagation represented by spatiotemporal source analysis: correlation with surgical outcome
- PMID: 24315019
- PMCID: PMC3933022
- DOI: 10.1016/j.eplepsyres.2013.11.006
Clinical value of magnetoencephalographic spike propagation represented by spatiotemporal source analysis: correlation with surgical outcome
Abstract
Objective: To investigate the correlation between spike propagation represented by spatiotemporal source analysis of magnetoencephalographic (MEG) spikes and surgical outcome in patients with temporal lobe epilepsy.
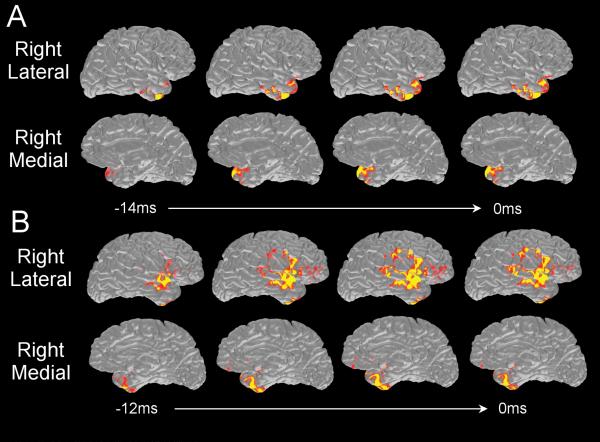
Methods: Thirty-seven patients were divided into mesial (n=27) and non-mesial (n=10) groups based on the presurgical evaluation. In each patient, ten ipsilateral spikes were averaged, and spatiotemporal source maps of the averaged spike were obtained by using minimum norm estimate. Regions of interest (ROIs) were created including temporoparietal, inferior frontal, mesial temporal, anterior and posterior part of the lateral temporal cortex. We extracted activation values from the source maps and the threshold was set at half of the maximum activation at the peak latency. The leading and propagated areas of the spike were defined as those ROIs with activation reaching the threshold at the earliest and at the peak latencies, respectively. Surgical outcome was assessed based on Engel's classification. Binary variables were created from leading areas (restricted to the anterior and mesial temporal ROIs or not) and from propagation areas (involving the temporoparietal ROI or not), and for surgical outcome (Class I or not). Fisher's exact test was used for significance testing.
Results: In total and mesial group, restricted anterior/mesial temporal leading areas were correlated with Class I (p<0.05). Temporoparietal propagation was correlated with Class II-IV (p<0.05). For the non-mesial group, no significant relation was found.
Conclusions: Spike propagation patterns represented by spatiotemporal source analysis of MEG spikes may provide useful information for prognostic implication in presurgical evaluation of epilepsy.
Keywords: Epilepsy surgery; Magnetoencephalography (MEG); Minimum norm estimate (MNE); Spike propagation; Temporal lobe epilepsy.
Copyright © 2013 Elsevier B.V. All rights reserved.
Figures


References
-
- Aghakhani Y, Rosati A, Dubeau F, Olivier A, Andermann F. Patients with temporoparietal ictal symptoms and inferomesial EEG do not benefit from anterior temporal resection. Epilepsia. 2004;45:230–236. - PubMed
-
- Alarcon G, Garcia Seoane JJ, Binnie CD, Martin Miguel MC, Juler J, Polkey CE, Elwes RD, Ortiz Blasco JM. Origin and propagation of interictal discharges in the acute electrocorticogram. Implications for pathophysiology and surgical treatment of temporal lobe epilepsy. Brain. 1997;120:2259–2282. - PubMed
-
- Assaf BA, Karkar KM, Laxer KD, Garcia PA, Austin EJ, Barbaro NM, Aminoff MJ. Magnetoencephalography source localization and surgical outcome in temporal lobe epilepsy. Clin. Neurophysiol. 2004;115:2066–2076. - PubMed
-
- Chen X, Sure U, Haag A, Knake S, Fritsch B, Müller HH, Becker R, Oertel WH, Bertalanffy H, Hamer HM, Rosenow F. Predictive value of electrocorticography in epilepsy patients with unilateral hippocampal sclerosis undergoing selective amygdalohippocampectomy. Neurosurg. Rev. 2006;29:108–113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
