

Blood flow characteristics in the ascending aorta after aortic valve replacement--a pilot study using 4D-flow MRI
- PMID: 24315151
- PMCID: PMC5099073
- DOI: 10.1016/j.ijcard.2013.11.034
Blood flow characteristics in the ascending aorta after aortic valve replacement--a pilot study using 4D-flow MRI
Abstract
Background: Aortic remodeling after aortic valve replacement (AVR) might be influenced by the postoperative blood flow pattern in the ascending aorta. This pilot study used flow-sensitive four-dimensional magnetic resonance imaging (4D-flow) to describe ascending aortic flow characteristics after various types of AVR.
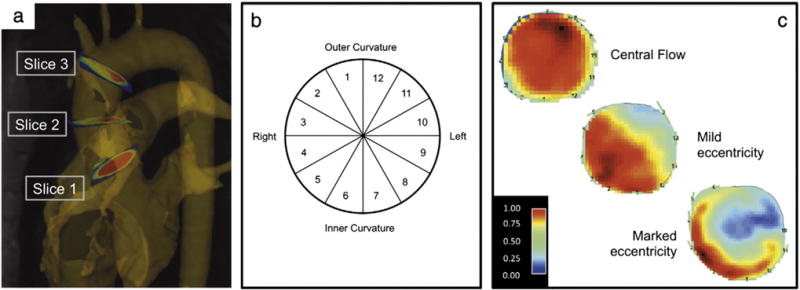
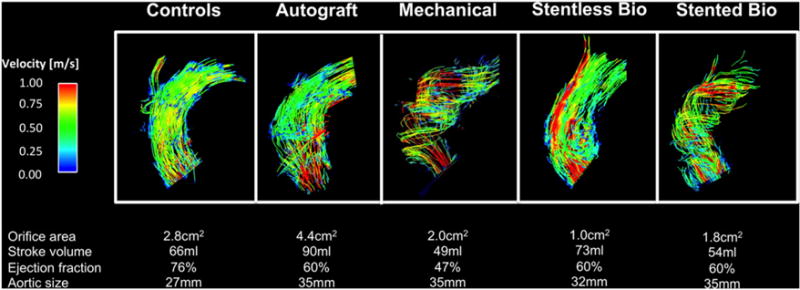
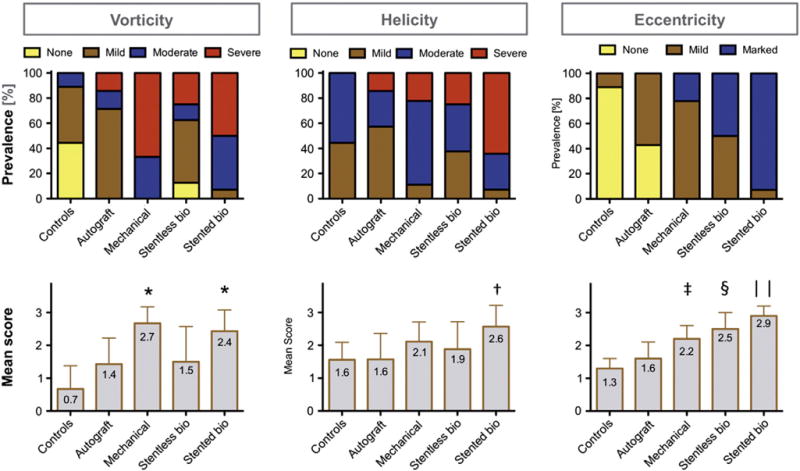
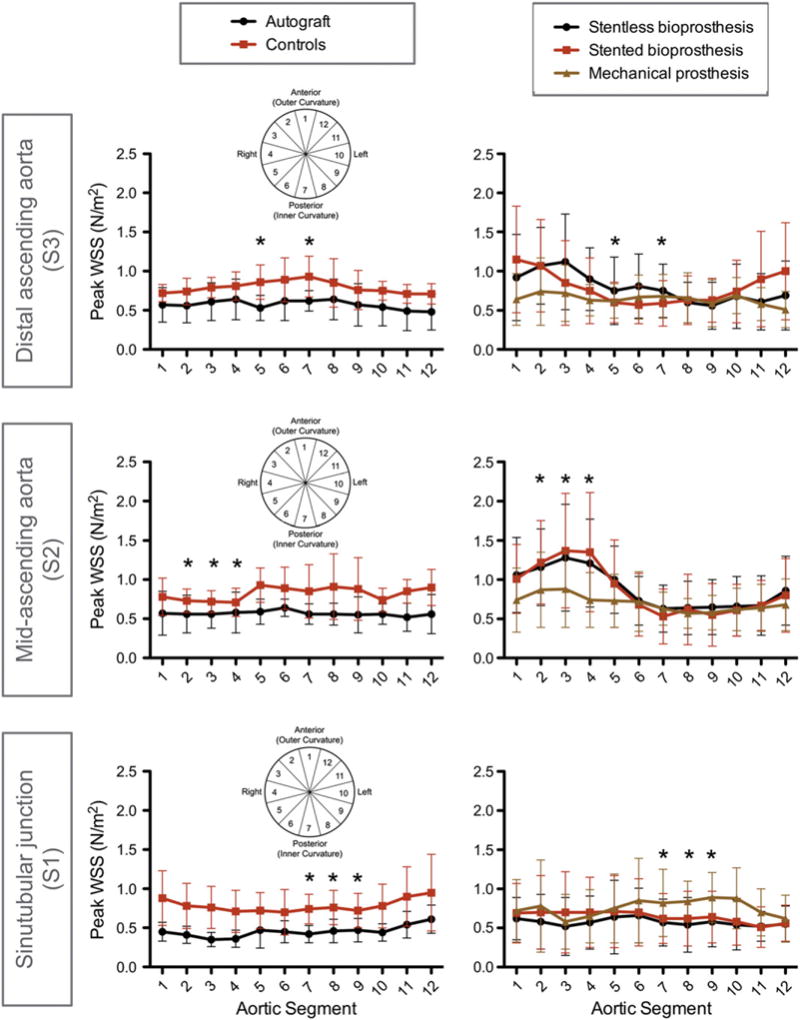
Methods: 4D-flow was acquired in 38 AVR patients (n=9 mechanical, n=8 stentless bioprosthesis, n=14 stented bioprosthesis, n=7 autograft) and 9 healthy controls. Analysis included grading of vortex and helix flow (0-3 point scale), assessment of systolic flow eccentricity (1-3 point scale), and quantification of the segmental distribution of peak systolic wall shear stress (WSS(peak)) in the ascending aorta.
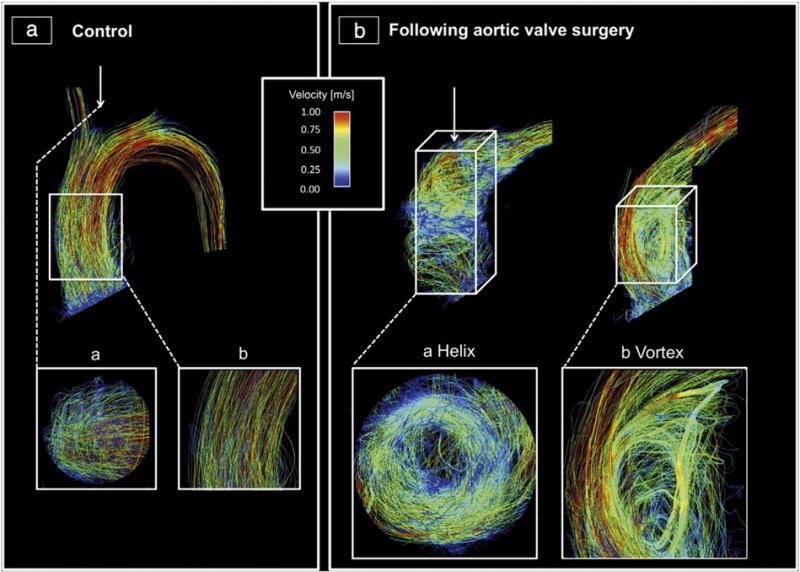
Results: Compared to controls, mechanical prostheses showed the most distinct vorticity (2.7±0.5 vs. 0.7±0.7; p<0.001), while stented bioprostheses exhibited most distinct helicity (2.6±0.7 vs. 1.6±0.5; p=0.002). Instead of a physiologic central flow, all stented, stentless and mechanical prostheses showed eccentric flow jets mainly directed towards the right-anterior aortic wall. Stented and stentless prostheses showed an asymmetric distribution of WSS(peak) along the aortic circumference, with significantly increased local WSS(peak) where the flow jet impinged on the aortic wall. Local WSS(peak) was higher in stented (1.4±0.7 N/m(2)) and stentless (1.3±0.7 N/m(2)) compared to autografts (0.6±0.2 N/m(2); p=0.005 and p=0.008) and controls (0.7±0.1 N/m(2); p=0.017 and p=0.027). Autografts exhibited lower absolute WSS(peak) than controls (0.4±0.1 N/m(2) vs. 0.7±0.2 N/m(2); p=0.003).
Conclusions: Flow characteristics in the ascending aorta after AVR are different from native aortic valves and differ between various types of AVR.
Keywords: 4D-flow; Aorta; Hemodynamics; Magnetic resonance imaging; Surgery; Valves.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Gaudino M, Anselmi A, Morelli M, et al. Aortic expansion rate in patients with dilated post-stenotic ascending aorta submitted only to aortic valve replacement long-term follow-up. J Am Coll Cardiol. 2011;58:581–4. - PubMed
-
- Botzenhardt F, Hoffmann E, Kemkes BM, Gansera B. Determinants of ascending aortic dimensions after aortic valve replacement with a stented bioprosthesis. J Heart Valve Dis. 2007;16:19–26. - PubMed
-
- Cozijnsen L, Braam RL, Waalewijn RA, et al. What is new in dilatation of the ascending aorta? Review of current literature and practical advice for the cardiologist. Circulation. 2011;123:924–8. - PubMed
-
- Malek AM, Alper SL, Izumo S. Hemodynamic shear stress and its role in atherosclerosis. J Am Med Assoc. 1999;282:2035–42. - PubMed
-
- Cecchi E, Giglioli C, Valente S, et al. Role of hemodynamic shear stress in cardiovascular disease. Atherosclerosis. 2011;214:249–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
