

Nexfin noninvasive continuous hemodynamic monitoring: validation against continuous pulse contour and intermittent transpulmonary thermodilution derived cardiac output in critically ill patients
- PMID: 24319373
- PMCID: PMC3844244
- DOI: 10.1155/2013/519080
Nexfin noninvasive continuous hemodynamic monitoring: validation against continuous pulse contour and intermittent transpulmonary thermodilution derived cardiac output in critically ill patients
Abstract
Introduction: Nexfin (Bmeye, Amsterdam, Netherlands) is a noninvasive cardiac output (CO) monitor based on finger arterial pulse contour analysis. The aim of this study was to validate Nexfin CO (NexCO) against thermodilution (TDCO) and pulse contour CO (CCO) by PiCCO (Pulsion Medical Systems, Munich, Germany).
Patients and methods: In a mix of critically ill patients (n = 45), NexCO and CCO were measured continuously and recorded at 2-hour intervals during the 8-hour study period. TDCO was measured at 0-4-8 hrs.
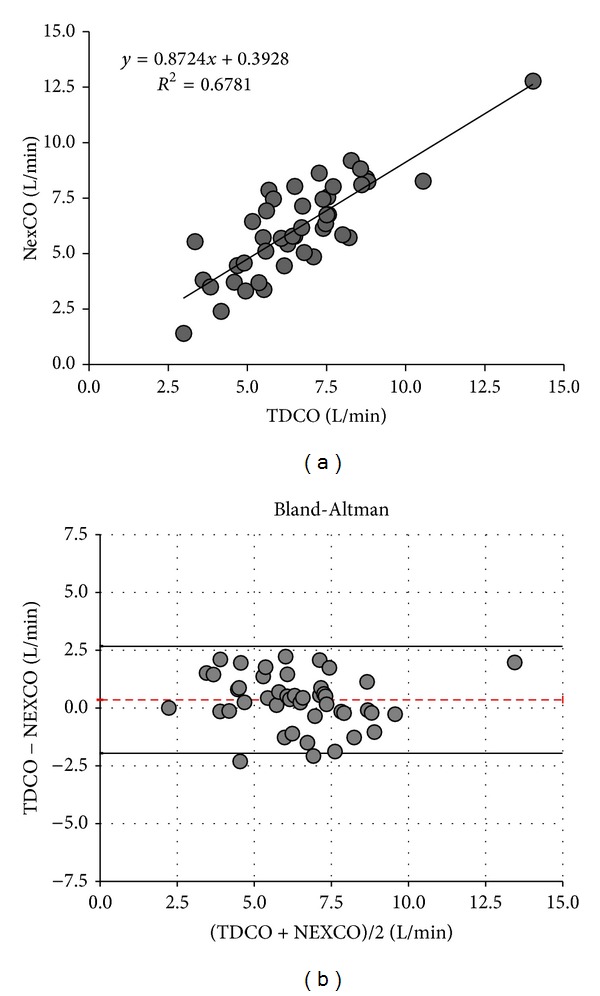
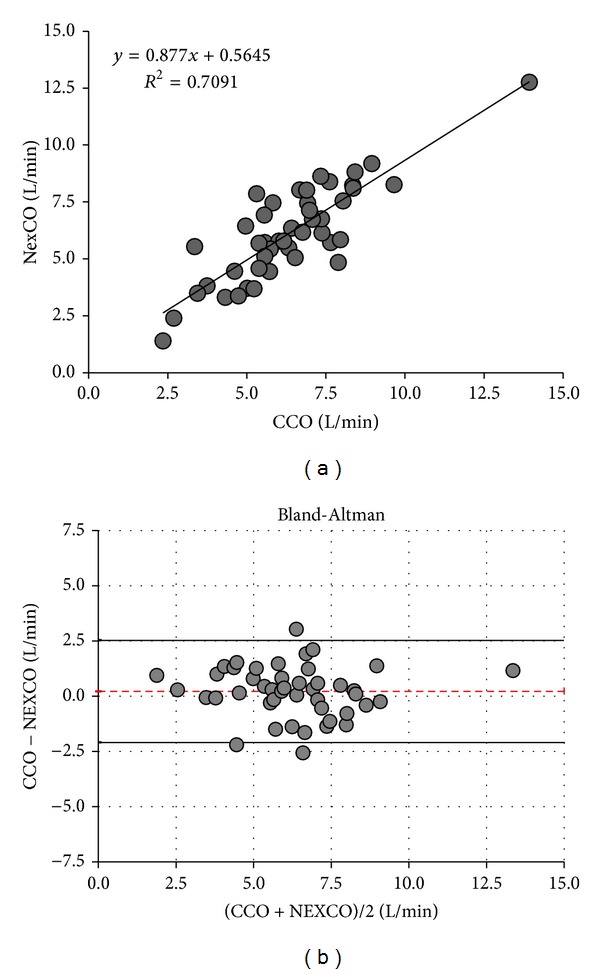
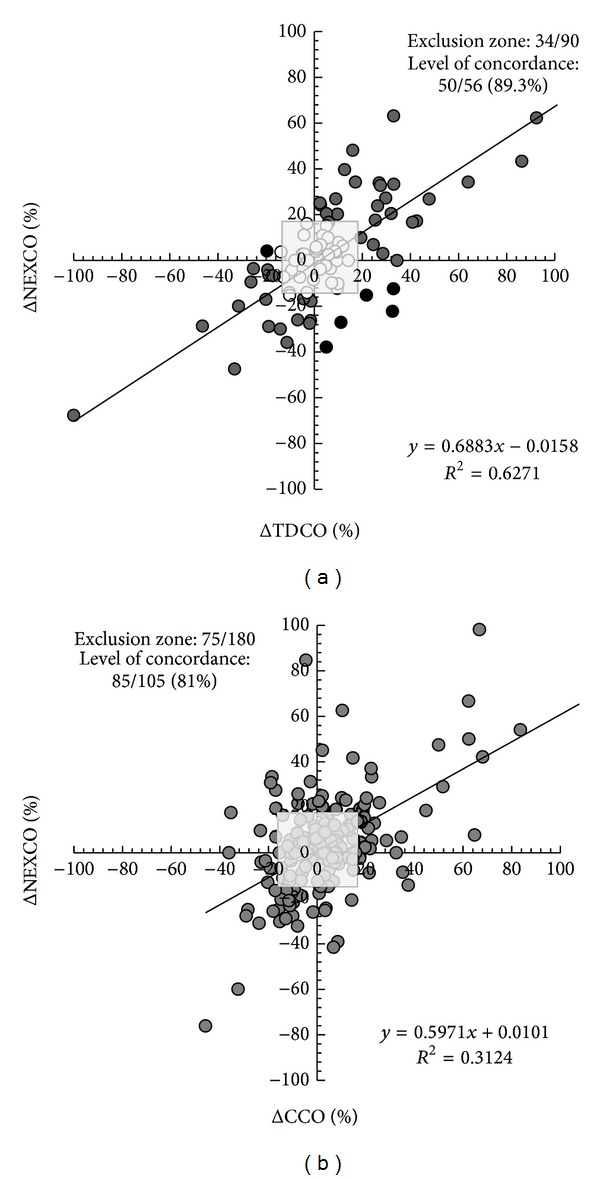
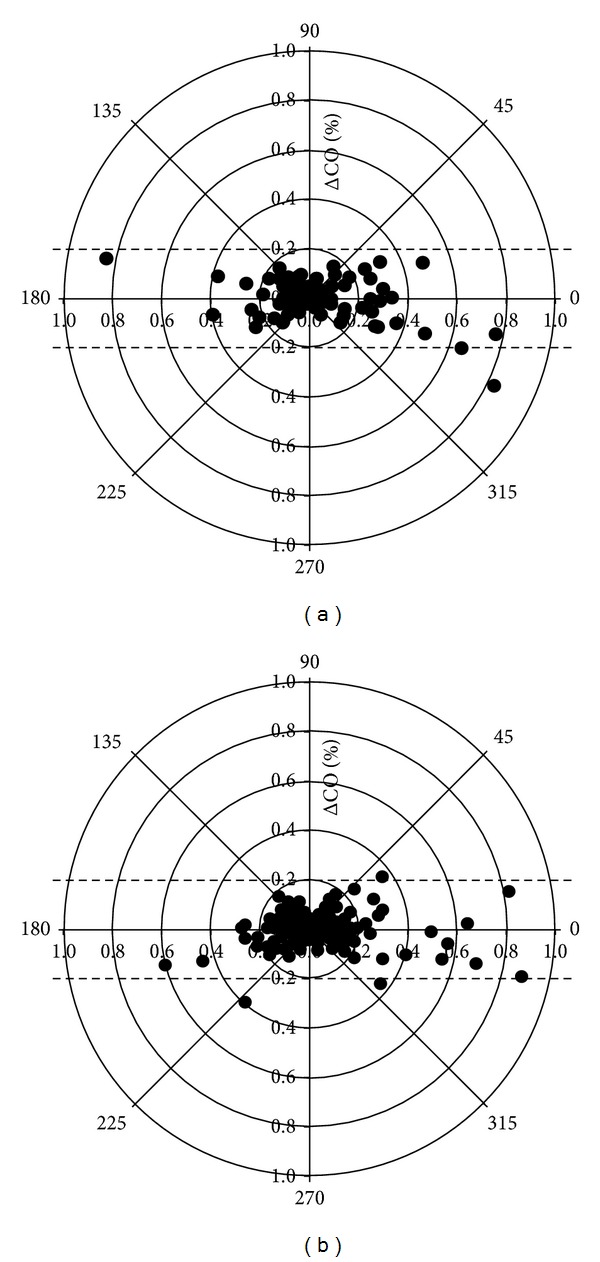
Results: NexCO showed a moderate to good (significant) correlation with TDCO (R (2) 0.68, P < 0.001) and CCO (R (2) 0.71, P < 0.001). Bland and Altman analysis comparing NexCO with TDCO revealed a bias (± limits of agreement, LA) of 0.4 ± 2.32 L/min (with 36% error) while analysis comparing NexCO with CCO showed a bias (±LA) of 0.2 ± 2.32 L/min (37% error). NexCO is able to follow changes in TDCO and CCO during the same time interval (level of concordance 89.3% and 81%). Finally, polar plot analysis showed that trending capabilities were acceptable when changes in NexCO (ΔNexCO) were compared to ΔTDCO and ΔCCO (resp., 89% and 88.9% of changes were within the level of 10% limits of agreement).
Conclusion: we found a moderate to good correlation between CO measurements obtained with Nexfin and PiCCO.
Figures
References
-
- Calvin JE, Driedger AA, Sibbald WJ. Does the pulmonary capillary wedge pressure predict left ventricular preload in critically ill patients? Critical Care Medicine. 1981;9(6):437–443. - PubMed
-
- Malbrain M, De Potter P, Deeren D. Cost effectiveness of minimally invasive hemodynamic monitoring. In: Vincent JL, editor. Yearbook of Intensive Care and Emergency Medicine. 2005. pp. 603–618.
-
- Michard F. Do we need to know cardiac preload? In: Vincent JL, editor. Yearbook of Intensive Care and Emergency Medicine. 2004. pp. 694–701.
-
- Oren-Grinberg A. The piCCO monitor. International Anesthesiology Clinics. 2010;48(1):57–85. - PubMed
-
- Genahr A, McLuckie A. Transpulmonary thermodilution in the critically ill. British Journal of Intensive Care. 2004;14(1):6–10.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
