

Gastroduodenal outlet obstruction and palliative self-expandable metal stenting: a dual-centre experience
- PMID: 24319458
- PMCID: PMC3844165
- DOI: 10.1155/2013/167851
Gastroduodenal outlet obstruction and palliative self-expandable metal stenting: a dual-centre experience
Abstract
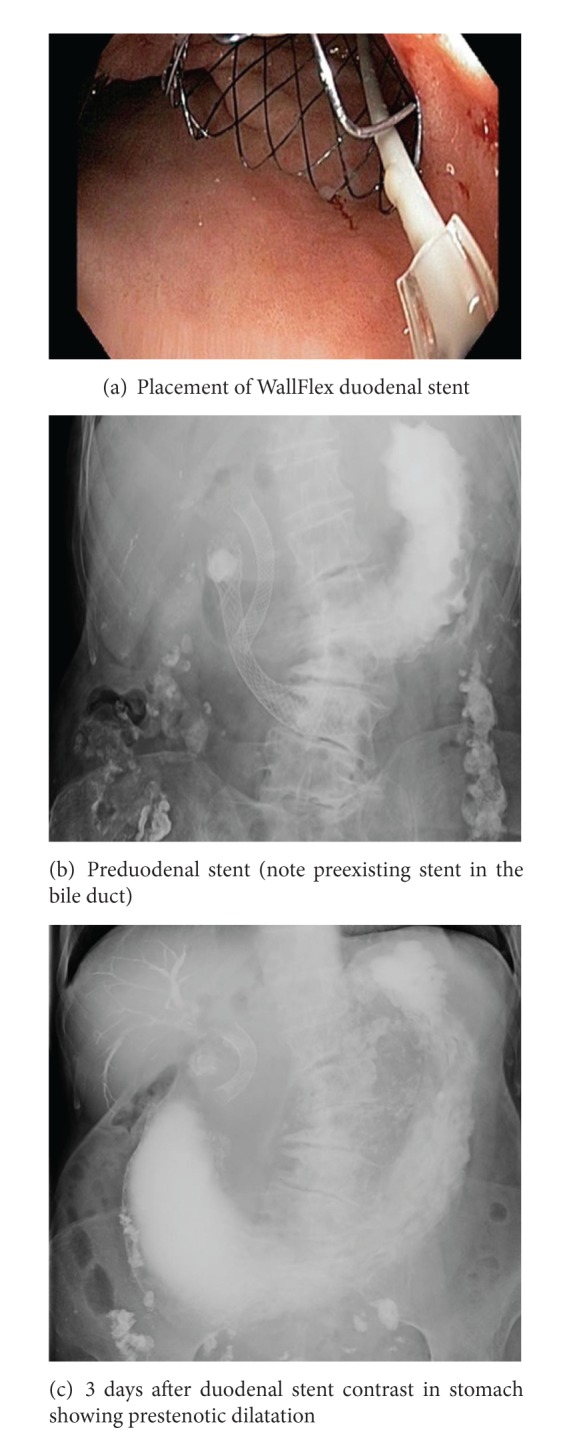
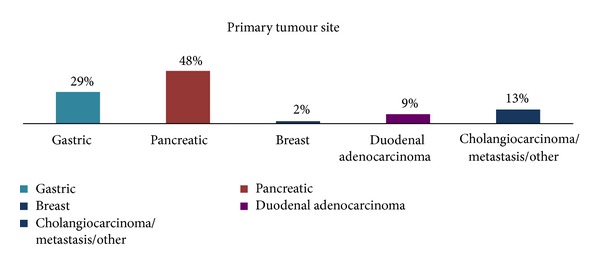
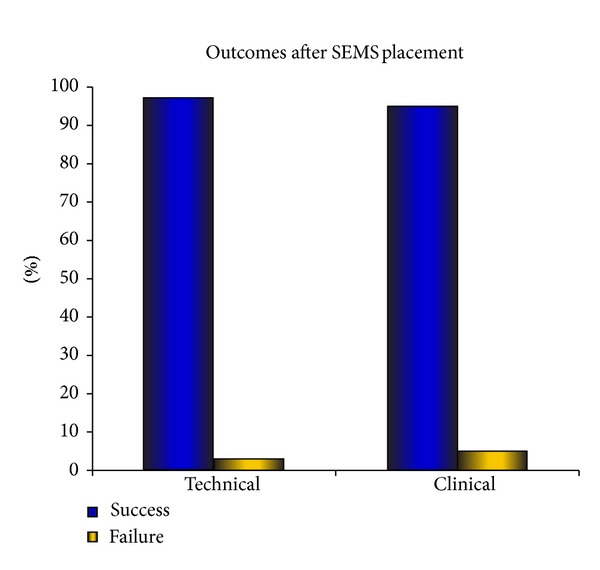
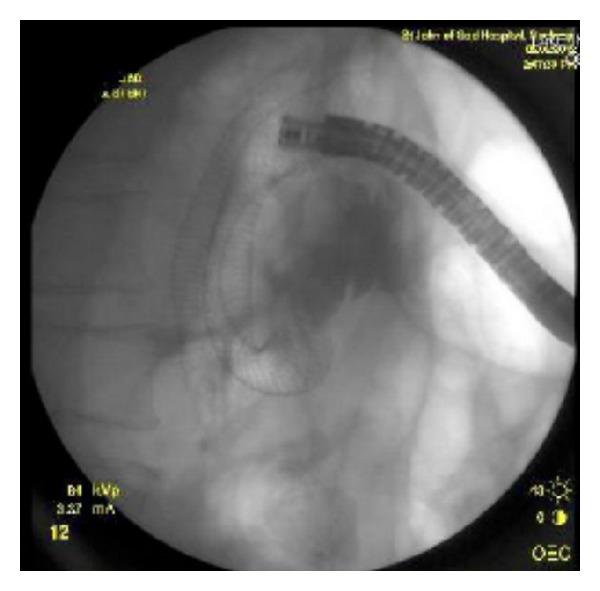
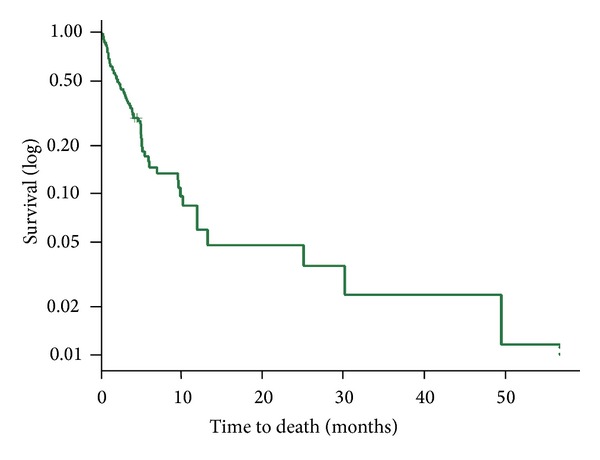
Background. Self-expandable metal stents (SEMs) are increasingly being utilised instead of invasive surgery for the palliation of patients with malignant gastroduodenal outlet obstruction. Aim. To review two tertiary centres' experience with placement of SEMs and clinical outcomes. Methods. Retrospective analysis of prospectively collected data over 12 years. Results. Ninety-four patients (mean age, 68; range 28-93 years) underwent enteral stenting during this period. The primary tumour was gastric adenocarcinoma in 27 (29%) patients, pancreatic adenocarcinoma in 45 (48%), primary duodenal adenocarcinoma in 8 (9%), and cholangiocarcinoma and other metastatic cancers in 14 (16%). A stent was successfully deployed in 95% of cases. There was an improvement in gastric outlet obstruction score (GOOS) in 84 (90%) of patients with the ability to tolerate an enteral diet. Median survival was 4.25 months (range 0-49) without any significant differences between types of primary malignancy. Mean hospital stay was 3 days (range 1-20). Reintervention rate for stent related complications was 5%. Conclusion. The successful deployment of enteral stents achieves excellent palliation often resulting in the prompt reintroduction of enteral diet and early hospital discharge with minimal complications and reintervention.
Figures
References
-
- van Heek NT, van Geenen RCI, Busch ORC, Gouma DJ. Palliative treatment in “peri”-pancreatic carcinoma: stenting or surgical therapy? Acta Gastro-Enterologica Belgica. 2002;65(3):171–175. - PubMed
-
- Kulke MH. Metastatic pancreatic cancer. Current Treatment Options in Oncology. 2002;3(6):449–457. - PubMed
-
- Weber CA, Decker RA, Puggioni A, Tom PM, Bendtsen D. Previously undiagnosed infiltrating lobular carcinoma of the breast presenting as a gastric outlet obstruction. The American Journal of Gastroenterology. 2001;96(12):3475–3477. - PubMed
-
- Spencer JA, Crosse BA, Mannion RAJ, Sen KK, Perren TJ, Chapman AH. Gastroduodenal obstruction from ovarian cancer: imaging features and clinical outcome. Clinical Radiology. 2000;55(4):264–272. - PubMed
-
- Adler DG, Baron TH. Endoscopic palliation of malignant gastric outlet obstruction using self-expanding metal stents: experience in 36 patients. The American Journal of Gastroenterology. 2002;97(1):72–78. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
